
United Nations System 22 September 2023
High-level Committee on Management (HLCM)
46
th
Session, 5-6 October 2023
UNICEF Global Supply and Logistics Hub, Copenhagen
UN System Workplace Mental Health and Well-being Strategy:
2024 and beyond Strategy
Introduction
1. The purpose of this agenda item is to present the proposed 2024 and beyond UN System
Workplace Mental Health and Well-being Strategy for approval by the HLCM. This paper includes:
a) Proposed 2024 and Beyond Mental Health and Well-being Strategy, its implementation guide
and scorecard, and the JIU recommendations with the corresponding scorecard indicators
(Appendix I); and
b) Proposed Strategy’s implementation staffing structure, location options, 2024 budget and
cost-sharing distribution model (Appendix II).
2. Significant progress was made with the 2018-23 UN System Workplace Mental Health and Well-
being Strategy
1
. While the Covid-19 pandemic had an impact on implementation, it also allowed
an increased understanding of the importance of mental health and well-being in the workplace.
3. It is critical we continue to act to create a mentally health working environment, which minimizes
the financial impact stemming from reduced productivity pertaining to poor mental health of
personnel and enables the UN to deliver on its mandates.
4. The HLCM endorsement of the Mental Health and Well-being Strategy for 2024 and beyond would
reflect the UN's ongoing high-level commitment to the mental health and well-being of UN
personnel and ensures we build on the progress made to-date.
5. The 2024 and beyond strategy builds on the foundations developed and move toward a sustainable
and integrated approach to mental health and well-being across the UN System.
6. We need to ensure a strategy is in place to guide evidence-based actions with a sustainable funding
model that supports UN Organizations to take appropriate action.
1
https://www.un.org/en/healthy-workforce/files/Strategy%20-%20full.pdf
CEB/2023/HLCM/30
CEB
Chief Executives Board
for Coordination

CEB/2023/HLCM/30
Page 2
7. The benefits of a system-wide approach have been demonstrated during the first phase of the
strategy as it allows for minimization of duplication of effort, a shared approach and a mechanism
to share lessons learnt.
8. The current strategy has been funded with voluntary contributions (cash and in-kind support)
9. The strategy addresses a number of recommendations made in the recent Joint Inspection Unit
(JIU) review into mental health policies and practices in the UN System
2
.
UN System Workplace Mental Health and Well-being Strategy (2018-23)
10. The first UN System Workplace Mental Health and Well-Being Strategy was approved by the
HLCM and subsequently launched by the Secretary-General in October 2018.
11. The 2018-2023 UN System Workplace Mental Health and Well-being Strategy aimed to:
a) Create a workplace that enhances mental and physical health and well-being;
b) Develop, deliver and evaluate high-quality psychosocial services everywhere that UN staff
work;
c) Welcome and support staff who live with mental health challenges; and
d) Ensure sustainable funding for mental health and well-being services.
12. A multi-agency, multi-disciplinary Implementation Board was established, and a P5 Global Lead
was appointed and commenced in 2019 to support the implementation of the strategy.
13. Significant progress was made following the launch of the 2018-23 Strategy:
a) The establishment of a governance mechanism with the multi-agency, multi-disciplinary
Implementation Board has enabled a system-wide approach;
b) The creation of quality control and reporting tools with the Mental Health and Well-being
Implementation Guide and Scorecard;
c) System-wide agreed upon best practices, as reflected in the new 2024 and Beyond Mental
Health and Well-being Strategy;
d) Education programs such as Lead and Learn which is free to all UN personnel, and outreach
events such as World Mental Health Month activities, has resulted in mental health literacy
has increasing at the UN. This allows for a robust discussion, at all levels, on the effects, both
positive and negative, our working environment can have on the mental health of personnel;
e) A variety of new data collection methods has shown the importance of mental health in the
workplace, particularly its effect on the productivity, morale and ability for the UN to deliver
on its mandate; and
f) Communication and engagement activities, particularly during World Mental Health Month.
14. A summary of progress made can be found in CEB/2023/HLCM/18.
15. Implementation of the strategy to-date has been funded with voluntary contributions (cash and
in-kind support from UN Organizations).
2
https://www.unjiu.org/sites/www.unjiu.org/files/jiu_ml_2023_1.pdf

CEB/2023/HLCM/30
Page 3
Proposed UN System Workplace Mental Health and Well-being
Strategy for 2024 and beyond
16. Evidence indicates that there are further opportunities for action. This evidence comes from:
a) Data from UN health surveys which indicates that the working environment impacts on the
mental health of UN personnel.
b) The 2023 Mental Health and Well-being Scorecard Report which points to distinct areas
where UN organizations can take further action, particularly related to prevention,
leadership and stigma reduction.
c) The JIU Review ‘mental health and well-being policies and practices in the United Nations
system organizations’, which clearly outlines the negative financial impacts of poor mental
health at the UN and the organizational risks posed by not taking a system wide approach.
d) The WHO/ILO Mental Health at Work Policy Brief
3
published in September 2022 identified
areas for action based on the latest evidence.
17. At its 44
th
meeting in October 2022 the HLCM approved the development of a strategy for 2024
and beyond.
18. Following the endorsement by HLCM, the draft 2024 and beyond strategy was) with input from:
• The Mental Health and Well-being Implementation Board;
• Senior leaders, the staff federations, human resources professionals and mental health
service providers;
• Data gathering using the UN Health Survey results, Scorecard data and staff union surveys;
and
• WHO/ILO colleagues who developed the Mental Health at Work policy brief.
19. The 2024 and beyond strategy (Appendix I)
• Builds on the existing strategy;
• Is guided by the WHO Workplace Mental Health Guidelines4 and WHO/ILO Workplace
Mental Health Policy Brief;
• Is accessible and ‘user-friendly’ for all personnel;
• Provides overall guidance that can be adapted to the needs of each UN Organization and
duty
• Is evidence-informed, culturally sensitive, and mindful of the unique circumstances that UN
personnel face; and
• Includes an implementation guide and updated scorecard (refer to Annexes I and II in
Appendix I).
3
https://www.who.int/publications/i/item/9789240057944
4
https://www.who.int/publications/i/item/9789240053052
CEB/2023/HLCM/30
Page 4
Proposed Staffing Structure, location options, 2024 Budget and cost-
Funding Model
20. At its 44th meeting in October 2022 the HLCM requested the Implementation Board to develop
a sustainable and long-term funding proposal.
21. Furthermore, JIU in paragraph 18 of its report on the review into mental health policies and
practices in the UN System i.18. “Furthermore, securing sustainable funding for coordinating the
implementation of the Strategy should be a priority, especially considering its second iteration.7
A more sustainable and predictable staffing and funding arrangement to support the
implementation of the Strategy across the United Nations system should be considered, especially
given the monitoring and reporting requirements, outreach and a new iteration of the Strategy to
be approved in 2023 with a view to commencing implementation in 2024.”
22. Resourcing requirements have been considered by the Implementation Board with a view to
maximizing return on investment and minimizing duplication of effort.
23. Appendix II contains the details of the resource proposal of the next iteration of the Strategy.
Conclusion
24. Implementation of the 2018-23 UN System Workplace Mental Health progressed as planned and
built a solid foundation for future success through the governance of the Implementation Board,
the system wide data collection of the Mental Health and Well-being Scorecard, and the proposal
of a system-wide funding model.
25. For the 2024 and beyond strategy, the Implementation Board endorsed the evidence informed
WHO/ILO model at outlined in their Mental Health at Work Policy Brief and focused resources on
preventing risks to mental health at work, promoting well-being and protecting mental health at
work and supporting personnel with mental health conditions.
26. The 2024 and beyond UN System Workplace Mental Health and Well-being Strategy represents
a significant step forward in the UN's commitment to promoting mental health and well-being
for its workforce. The comprehensive data gathering and consultation process ensured that the
strategy is grounded in the needs of personnel and reflects best practices in workplace mental
health and well-being.
27. Recommendations have been made to ensure funding is available for the implementation of the
2024 and beyond strategy.
Proposed actions for the HLCM
28. The HLCM is invited to:
a) Approve the 2024 and Beyond Mental Health and Well-being Strategy;
b) Approve the Strategy’s implementation guide;
c) Approve the Strategy’s scorecard and request the Implementation Board to report on annual
basis;
d) Approve the staffing structure for an initial period of three years;
e) Approve the budget for the year 2024; and
f) Approve the cost-sharing distribution model.

0
SUMMARY / OVERVIEW
The UN System Workplace Mental Health and Well-being Strategy (the Strategy) is designed to assist the
United Naons to create a working environment that is conducive to good mental health and ensures that
support is available when it is needed. The Strategy provides a roadmap to create “an inclusive,
sustainable work environment where mental health and well-being is embedded in the organizaonal
culture and systems - where each and every one belongs, is valued, nurtured and thrives, ensuring an
ecient workforce delivering on our promise of a beer world”.
WHO states that mental health is more than the absence of mental health condions. Rather, mental
health is a state of mental well-being that enables people to cope with the stresses of life, to realize their
abilies, to learn well and work well, and to contribute to their communies.
UN personnel, in all locaons, can nd themselves working in challenging situaons. These challenges can
be due to pressure and deadlines, being in a high-risk duty staon or the result of isolaon from family
and being away from their country of origin. Successive surveys have shown that UN personnel report
high levels of symptoms consistent with poor mental health. Our working environment can play a direct
role in this. Good working condions protect mental health. Work can also be good for us, healthy working
condions can protect mental health. UN personal, in all locaons, may be living with mental health
condions irrespecve of work as a contributory factor.
The costs of inacon are high. Poor mental health leads to reduced producvity, sta absences and
turnover, and risks our ability to deliver on our mandates. There are also costs to our personnel, their
families and communies as they navigate the impact of symptoms of poor mental health and the eect
this can have on their lives.
The acons we take now can have a real and posive impact on the mental health of our personnel.
This strategy builds on gains made in the implementaon of the rst Strategy (2018-23), and takes into
account the latest evidence based, data collected from UN survey’s and the 2023 JIU review into mental
health policies and pracces within the UN.
The Strategy is guided by the WHO/ILO Mental Health at Work policy brief
1
, which calls for organizations
to act:
1. Prevenng risks to mental health at work
2. Promong well-being and protecng mental health at work
3. Supporng personnel with mental health condions
Each of these three pillars are supported by indicators to help organizaons measure success, technical
guidance when needed, as well as suggesons for allocaon of responsibility.
1
This is an evidence-based policy brief based on the WHO guidelines on mental health at work
hps://www.who.int/publicaons/i/item/9789240053052

1
Essenals for eecve implementaon
1. Everyone has a role to play
This is a shared responsibility, requiring collecve eort, with collecve acon, for a collecve
benet.
2. It is not one size-ts all
Each UN Organizaon has its own organizaonal culture and will determine how to implement the
strategy.
3. System-wide coordinaon and support
This minimizes duplicaon of eorts through shared resources, seng common standards and
sharing good pracces. Good pracces are occurring across the UN system, and it is important
that a collaborave approach be taken so we can learn from each other.
4. Integrang mental health and well-being into policies and pracces
As this is not a stand-alone acvity, it needs to be mainstreamed into the way we work and
integrated into workplace pracces and behaviours.
5. Leadership support is crucial
Senior leaders are asked to be public champions of the strategy, to take responsibility to reduce
of workplace risks, to enable acons to promote and protect a mentally healthy workforce, and
ensure support is available for personnel living with mental health condions, when needed.
6. The role of managers is pivotal
Managers need the skills to create a healthy working environment, reduce risks within their teams,
and to support sta to access help when needed. They also need to know how to take care of
their own mental health.
7. Data informed decision making
Data related to mental health and well-being about the UN Organizaons allows us to understand
the unique issues we face and where to focus acons.
8. Taking acon to support mental health and well-being is possible
Provision of an implementaon guide and an accompanying scorecard guides organizaons in
what acons should be taken and how to measure this.
BACKGROUND
The 2018-23 Mental Health and Well-being Strategy
The first UN System Workplace Mental Health and Well-being Strategy was launched by the Secretary
General in October 2018. This Strategy was developed after a Global Well-Being Survey, completed by
over 17,000 United Nations staff members across 11 United Nations Organizations in 2015, revealed that
approximately half of all United Nations staff members who responded to the survey reported

2
experiencing symptoms that can be interpreted as being consistent with serious mental health
conditions.
The implementation of the 2018-23 Strategy was overseen by a system-wide, multi-disciplinary, multi-
agency Implementation Board, which reported to the High-Level Committee on Management (HLCM) via
the Human Resources (HR) Network.
Significant gains were made during the implementation of the first strategy and the 2024 and beyond
Strategy builds on these gains.
Development Process
The Strategy was developed by the system-wide, multi-disciplinary, multi-agency Implementation Board.
Key inputs in the Strategy’s development include lessons learnt from the 2018-23 strategy, the WHO/ILO
Mental Health at Work policy brief, inputs from personnel and the recommendations from the Joint
Inspection Unit (JIU) review into UN system-wide mental health policies and practices. After this
information was compiled, an in-person retreat with the Implementation Board was held in 2023 to agree
on key elements of the strategy. In addition, a multi-disciplinary working group, chaired by the Global
Lead, oversaw the drafting of the strategy and its related annexes.
The State of Mental Health in the UN System
The JIU report highlighted that baseline data, and subsequent studies have confirmed, that UN System
personnel experience a number of psycho-social risk factors at work and report high rates of symptoms
consistent with a mental health condition.
The report noted that sick leave and disability data provided by participating organizations show that this
is an increasing trend. This is of particular concern as associated costs are high. Poor mental health leads
to reduced productivity and risks our ability to deliver on our mandate. The poor mental health of
personnel has resulted in increased costs for UN system organizations, personnel, families and
communities. This is not an isolated trend. Over the last 10 years, several surveys have shown that the
mental health of personnel has been declining.
This impacts productivity and has subsequent financial implications. In addition, there are personal cost
for our staff and their families.
Based on JIU findings, the trend of declining mental health poses two main economic risks to the UN,
the increasing cost of sick leave due to mental health diagnoses and the increase of costs due to
disability pension claims.

3
1. Increased sick leave
Every year, the percentage of sick leave rates associated with a mental health diagnosis is
increasing. This not only represents a cost reflected in the lost productivity of the individual on
leave, but negatively impacts teams and programme delivery if policies and workplace practices
are not enacted. Based on certified sick leave data, provided to JIU by participating organizations,
in 2021 nearly 20 per cent of all sick leave taken was attributable to mental health, up from 16
per cent in 2017. Absence and poor implementation of return-to-work policies and mechanisms
supporting them, such as partial and temporary disability, reasonable accommodations, talent
solutions, etc., increase the negative impact of sick leave for mental health reasons on individuals
and organizations.
Source: prepared by JIU on the basis of information provided by the United Nations Secretariat, FAO, UNHCR, UNICEF, WFP and WIPO.
2. Increased disability claims
Based on data provided provided to the JIU from the Legal Office of the United Nations Joint Staff
Pension Fund (UNJSPF), the proportion of disability cases granted to United Nations System staff
for mental health reasons has increased, from 37.5 per cent for the 2016-2017 biennium to over
45 per cent for the 2020-2021 biennium. Moreover, from the 2010-2011 biennium to 2020-2021,
the number of disability cases with a psychiatric diagnosis has increased over 158 per cent.
Information regarding disability cases and percentage of cases with psychiatric diagnoses (2016-2021,
by biennium)
Biennium
Cases where disability
benefits were granted
Cases with psychiatric
diagnosis
Percentage of cases with
psychiatric diagnosis
2016-2017
245
92
37.5
2018-2019
339
153
45.1
2020-2021
262
119
45.4
Total 2016-2021
846
364
43
Source: prepared by JIU on the basis of informaon provided by the United Naons Joint Sta Pension Fund (2022)
19.5%
16%
0 100,000 200,000 300,000 400,000 500,000
2021
2017
Sick leave days Sick leave days for mental health reasons

4
THE STRATEGY
The Strategy is aligned with the WHO/ILO Mental Health at Work policy brief which calls for organizations
to act to:
1. Prevent risks to mental health at work
2. Promote well-being and protect mental health at work
3. Support personnel with mental health condions
They also idened a number of cross-cung issues to create an enabling environment.
System-wide action
This is a system-wide strategy and global efforts will be undertaken to support UN Organizations to take
action. An implementation guide and scorecard have been developed to guide the work of UN
Organizations. The Strategy provides the overarching framework to address workplace mental health and
well-being. How the Strategy is implemented may vary across organizations.
Supportive actions taken the system-wide level will include:

5
• Streamlined evaluation and reporting
• Data collection and analysis
• Integration with other system-wide strategies
• Development of policies, tools and learning products that can be adapted by UN Organizations to
share resources required to develop products and programmes individually
• Undertake communication and change management activities, including campaigns, multimedia
and digital products and events
• Advocacy and strategic support for decision makers to implement the strategy
• Provision of guidance to UN Organizations on how to implement the strategy
Organizational action
UN Organizations are called to develop a Mental Health Action Plan. This could be standalone or
integrated within existing mechanisms, such as occupational health and safety plans.
An Implementation Guide (Annex I) has been developed to assist organizations in this process. An
assessment of needs will inform development of a plan. The implementation guide recommends ensuring
a leader has overall responsibility, the establishment of a multi-disciplinary working group and the
development of a tailored action plan with agreed deliverables. This should be based on the indicators
across three pillars: Prevent, Promote and Support.
A scorecard (Annex II) has been developed with three indicators for each pillar. Some organizations may
have already acted for each of the indicators, others may need to prioritize their starting point. The
strategy does not present timelines or recommend which indicators to commence with as organizational
circumstances vary. It is important to initiate the new actions and reinforce already existing activities in
line with a long-term strategic plan, setting out organization-specific priorities and implementing them in
a consistent manner.
UN Organizations will be held accountable via reporting on progress against indicators on an annual basis.
UN Organizations will need to ensure that resources are allocated to implement the action plan, including
the time required by relevant personnel is considered and added in their workplans.

6
Key Pillars and Indicators
Prevent
Promote
Support
1. Risk Assessment (Prevention
& mitigation)
3. Manager Training
7. Enabling Dignified Work
2. Policy & Practice
Mainstreaming
4. Stigma reduction activities
8. Access to psychosocial
support
5. Mental Health Literacy
training
9. Quality control for
psychosocial support
6.Implemention of well-being
initiatives
Cross cutting
10. Leadership
11. Reporting
12. Participation
Overview
1. Preventing poor mental health
Prevention requires an organizational approach to assessing and mitigating psycho-social risks. Actions
can be taken to ensure policies and practices consider workplace factors that can lead to poor mental
health. The WHO/ILO Policy brief outlines 10 psychosocial risks and interventions that can be taken to
mitigate them (see Annex III). UN data has highlighted four areas that need particular focus:
• Work-life harmony / workload management
• Job control
• Communication and interpersonal relationships
• Manager support
Actions need to take into consideration the lifecycle of personnel engagement from attracting candidates,
recruitment, on-boarding, learning, performance management, career development though to
retirement.
Key actions that can be undertaken under this pillar are:
• Incorporate mental health and well-being considerations into people management policies and
relevant practices (such as recruitment, on-boarding and people management)
• Undertake an assessment of psycho-social risks and develop a mitigation plan. The mitigation
plan should focus on practical measures that can be taken to manage risks identified. Examples

7
of this could include a focus on work planning and strategies to manage work overload and
initiatives to reduce incivility in the workplace.
2. Promote and protect mental health
The focus of this pillar is to increase understanding of mental health and well-being, how to promote good
mental health and well-being and how to encourage behaviours to support this change. This includes
organizaons providing conducive conditions for individuals to take action for the benefit of their mental
health.
Key actions that can be undertaken under this pillar are:
• Training and skill development for managers possess the skills to create a healthy working
environment
• Undertake stigma reduction activities that create conditions that enable personnel experiencing
mental health conditions to fully express their potential and meaningfully contribute to the work
of the UN Organization
• Provide mental health literacy programmes for all personnel
• Implement well-being initiatives (such as stress management, encouraging physical activity and
health promotion activities)
3. Support personnel with mental health conditions
Everyone needs support at different times. This is particularly critical for personnel experiencing poor
mental health. Personnel should have access to quality mental health care both through UN services and
via appropriate insurance with reasonable coverage.
Policies and practices should also be in place to allow reasonable accommodations to be made where
needed and robust return-to-work policies that ensure individuals and teams are supported to return
after absence due to a mental health condition.
Key actions that can be undertaken under this pillar are ensuring:
• reasonable accommodation and return-to-work policies and support are in place and that key
personnel are knowledgeable on what good support for personnel with mental health conditions
should entail
• access to psycho-social support through internal, shared and/or external resources including
insurance products
• the United Nations Staff Stress Counsellor Group (UNSSCG) report “Guidance on Professional
Standards for UN Counsellors” is followed

8
Cross-cutting issues
To support actions undertaken in the key pillars, cross cutting issues have been identified and will be
critical to success at an organizational level. While the WHO/ILO Policy outlines several other cross cutting
issues, these are the ones identified to be prioritized within the UN:
• leadership
• reporting
• participation
Leadership
Leadership buy-in and advocacy is required to enable a successful change process within an organization.
This means that the head of the organization openly advocates for mental health and well-being, behaves
in a manner that models and promotes healthy workplaces and ensures that appropriate resources are
allocated.
Reporting
UN Organizations will be asked to complete the scorecard on an annual basis, indicating where progress
has been made against their action plans. Initially, this will mean specifying what indicators the
organization has already met. In 2026, year 3 of the Strategy, a more robust approach will be taken, and
organizations will be requested to provide evidence and evidence-based information. Organizations are
also encouraged to gather and analyze mental health and well-being related data to guide actions and
monitor changes.
Participation
Participation focuses on ways that individuals and organizations can support the strategy. This includes
individuals with lived experience taking part in decision making processes, organizations providing focal
points for the Implementation Board, and allocating system wide resources for a global coordination
mechanism.
WHO IS RESPONSIBLE
We all can and should take action to support our own well-being and create a healthy working
environment. It is imperative that no one individual, position or department/office is seen to be
responsible for mental health and well-being in the workplace. The emphasis in this phase of the Strategy
is for everyone within the UN System to possess the skills to act for themselves and for their role and that
their organization and the UN System supports them to achieve change.
The WHO/ILO policy brief asks for actions to be taken on three levels: organizational, managerial, and
individual. As the Strategy suggests a mainstreamed multi-faceted approach, this will require
organizations to own and lead the implementation at multiple levels and through integrative processes.
Implementation of the Strategy is overseen by a system-wide, multi-disciplinary, multi-agency Board. The
Board reports to the HLCM via the HR Network.

9
Mental health and well-being is not a stand-alone issue. Action taken in many areas can have an impact
on mental health. Given this, the Board works with alignment and in collaboration with other relevant
bodies, such as the Occupational Health and Safety (OH & S) Forum, UN Staff Counsellors Group, the
Critical Incidence Stress Working Group, Staff Federations, UN Medical Directors, and the HR Network.
MEASURING SUCCESS
Success will be measured based on actions taken across the UN System as outlined in the scorecard.
Individually, UN Organizations will be able to compare their scorecard results against those of the whole
system.
To facilitate these required actions, system-wide thematic working groups will be set up that report to the
larger Implementation Board. The Implementation Board will then report annually on progress made to
the HLCM.
Annex IV contains the JIU recommendaons with the corresponding scorecard indicators.

10
Annex I
IMPLEMENTATION GUIDE
INTRODUCTION
The United Naons System Workplace Mental Health and Well-being Strategy (hereaer, ‘The Strategy’)
aims to create “an inclusive, sustainable work environment where mental health and well-being is
embedded in the organizaonal culture and systems -where each and every one belongs, is valued,
nurtured and thrives, ensuring an ecient workforce delivering on our promise of a beer world.”
As a supporng document to The Strategy, this Implementaon Guide (hereaer, ‘The Guide’) serves to
assist UN organizaons to mainstream psychosocial health and well-being into the culture of the United
Naons. The Strategy’s focus on creang a healthy workplace is underpinned by specic administrave
and process related indicators which will facilitate this change.
Recognizing that this is a workplace mental health and well-being document, these iniaves focus on the
workplace. This includes a focus on preventave measures, investment in mental health and well-being
programmes, educaon to reduce sgma, and ensuring that there is equal access to quality psychosocial
support as directed in The Strategy.
While The Guide focuses on collecng data for the three pillar areas of Prevent, Promote and Support (as
outlined in The Strategy), other acvies may also form part of an overall Acon Plan depending on the
needs of your organizaon. Recognizing that not every Pillar Indicator is equally applicable to every United
Naons enty, these indicators are not meant to compare groups, but instead create benchmarks
Organizaons can use to measure progress.
As shown in the Scorecard, many of the acons organizaons are being asked to take, involve a variety of
departments and speciales. This holisc approach will focus on working together, innovave soluons,
and an understanding that we can all take responsibility for improving the environment in which we work.
We all have a role to play in improving mental health and well-being at the UN.
THE ROLE OF THE ORGANIZATION
Comparison studies have shown that the reported levels of symptoms consistent with mental health
condions are higher in the UN (at approximately 50%) than in the general populaon.
2
Successive Sta
Well-being Surveys have highlighted that the longer people work for the United Naons the more likely
they are to experience negave mental health outcomes. Anxiety, depression, post-traumatic stress, and
hazardous drinking negatively impacts the quality of life of thousands of UN employees and costs the
Organization millions of dollars every year.
Structuring the workplace, working condions and workplace culture to put people rst can have a
signicant impact on the mental health and well-being of personnel. According to the World Health
Organizaon and Internaonal Labour Organizaon, many organizaonal factors inuence the mental

11
health of employees. These issues include poor communicaon and management pracces, limited
parcipaon in decision-making, long or inexible working hours and lack of team cohesion.
Despite current investment, there is an opportunity for improvement within the UN organizational mental health
and well-being approach. The Guide asks UN partners to influence change in 3 main areas. Recommended
actions are based on WHO’s “Guidelines on Mental Health at Work”. These guidelines, along with WHO/ILO’s
‘Mental Health at Work Policy Brief’ outline three key pillars, along with a number of cross-cutting actions.
1. Preventing risks to mental health at work
2. Promoting well-being and protecting mental health at work
3. Supporting personnel with mental health conditions
Key indicators have been identified for each of these pillars and can be found in the accompanying Scorecard.
Indicators are supported by actionable requirements which will be reported on yearly to HLCM. The Mental
Health and Well-being Scorecard will be the tool used for evaluation at the HLCM level.
To support actions undertaken as part of the key pillars, cross cutting issues have been identified which will be
critical to success. The cross-cutting issues that are included in the strategy are leadership support, reporting
structure and participation at all levels.
These thematic areas will serve as a foundation to achieve the overall goal of creating an environment that
enables good mental health and well-being, facilitates the ability of personnel to improve their resilience and
ensures targeted quality intervention is available for those seeking help.
To further these efforts, organizations will be asked to develop a Workplace Mental Health and Well-being Action
Plan, based on principles found in The Strategy. Keeping in mind that the size and resources of entities vary,
partners will be asked to tailor their plans to fit their specific needs and available funding. For some organizations,
The Guide will serve as a first step, while for others it is an opportunity to review their existing plans.
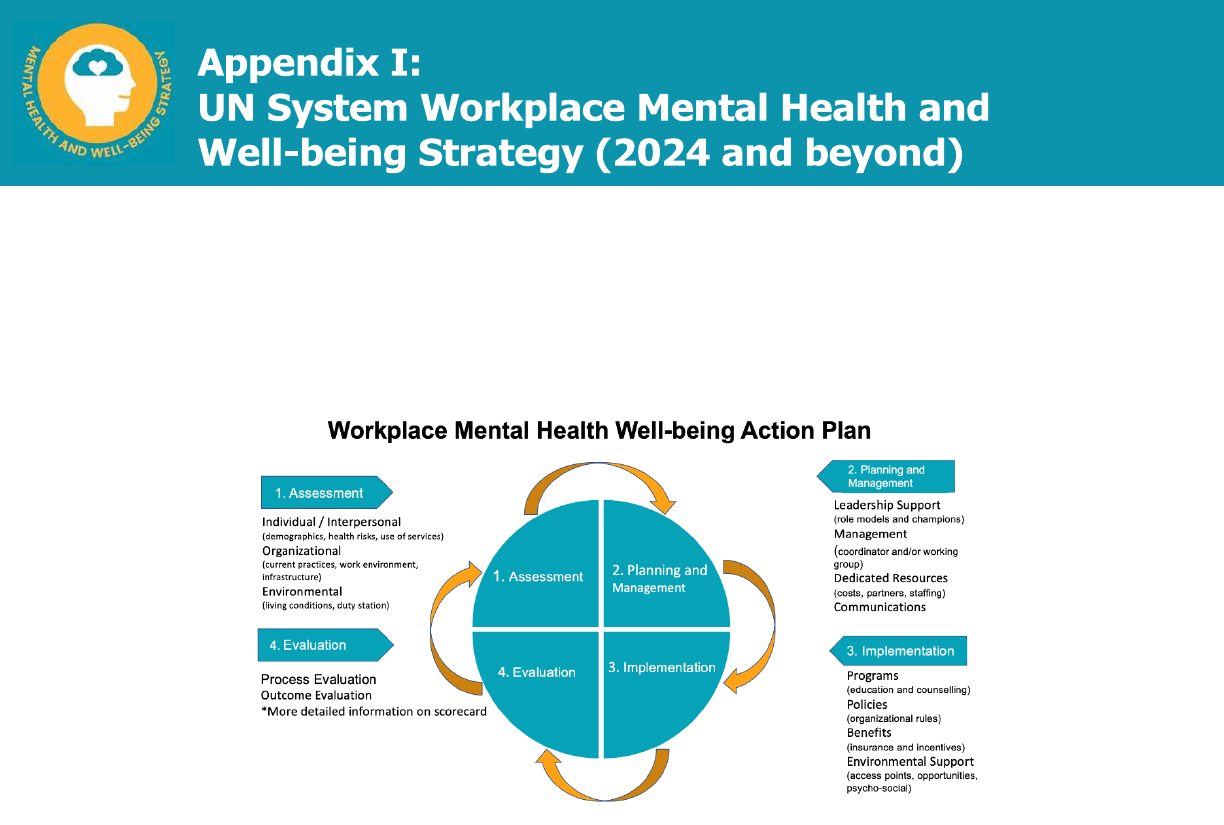
DEVELOPING A MENTAL HEALTH AND WELL-BEING ACTION PLAN
A Workplace Mental Health and Well-being Plan refers to a coordinated and comprehensive set of
strategies which include programmes, policies, benets, environmental support, and links to resources
designed to meet the mental health and well-being needs of all personnel.
3
The systemac process of building a Workplace Mental Health and Well-being Plan emphasizes four main
steps:
3
hps://www.cdc.gov/workplacehealthpromoon/model/index.html
12
Step 1 – Workplace Assessment
Step 2 – Planning
Step 3 – Implemenng
Step 4 – Determine impact through evaluaon
Step 1- Workplace Assessment
In the rst step, data is collected to assist organizaons to decide where to focus resources. There are
three data collecon levels to consider which cover the key areas of people, programmes, and inial
funding. Ideally, assessment team members should include people with lived experience.
• Interpersonal – elements of personnel's workplace network which includes relaonships with
managers and coworkers.
• Organizaonal – elements of the workplace structure, culture, pracces and policies such as
benets, health promoon programmes, work organizaon, and leadership and
management support for workplace well-being iniaves
• Environmental – elements of the physical workplace such as facilies and sengs where
employees work as well as access and opportunies for health promoon provided by the
surrounding duty staon.
Data sources for this assessment may include, but are not limited to psychosocial assessment tool, sick
leave data, use of EAP or counseling services by topic, job sasfacon surveys, UN-Wide Health Survey,
internal data collecon methods (surveys, quesonnaires, personnel inputs).

13
Step 2- Planning
During this phase resources are idened based on the priories idened in step one. These resources
may include:
• Senior leadership- individuals who will serve as role models, communicaon leaders and
champions within management.
• A workplace coordinator/focal point or working group to oversee the plan.
• Dedicang the nancial resources necessary to execute the plan.
• Creang a communicaons strategy to inform all personnel about priories, resources, and how
to join the eort.
Examples of Well-being Planning Group TORs can be found on the UN Healthy Workforce website
Step 3 – Implemenng the Plan
It is important for Mental Health and Well-being Plans to have acons across all of the key pillars and
indicators outlined in Annex I. These may include:
1. Mental Health and Well-being related policies and pracces – formal or informal wrien
statements that are designed to protect or promote the mental health and well-being of
personnel. Supporve policies aect large groups of personnel simultaneously and impact on the
working environment. Examples may include return-to-work policies for those coming back aer
experiencing a mental health condion, SOPs for reasonable accommodaons, and policies that
allow for greater autonomy for workload management, telecommung, and work-life harmony.
2. Mental Health and Well-being programmes – this can include training and educaon (such as the
Lead and Learn Programme or stress management) and access to counseling services- either
internal or external.
Step 4 – Determine Impact through Evaluaon
The evaluaon stage of the project is important for two reasons. First, it allows for informaon to be
gathered on ways in which the plan can be improved over me. Second, the evaluaon is a way to dene
the value of the plan to senior management.
There are 4 key areas for inclusion in your evaluaon which are reected in the Scorecard. These areas are
based on the 3 key pillars and cross cung secon outlined in the UN Workplace Mental Health and Well-
being Strategy. The following areas can be used in all stages of the project including to inform inial data
collecon, assist with creang the plan and nally implementaon and evaluaon.
The Scorecard will be the tool used for evaluaon at the HLCM level.

14
Annex II:
INDICATORS AND SCORECARD
The challenging work that UN personnel undertake, oen under high pressure and in dangerous locaons,
makes it imperave that our workplace is a safe place.
This means that acon is taken to create a healthy workplace culture, policies and pracces are in place
to support this, managers are trained to understand mental health and well-being, individuals are provided
with the tools they need to stay healthy, and support is provided for those in need.
Organizaons are encouraged to take acon in as many of these domains as possible. However, not all
indicators are appropriate for all organizaons. We understand that dierent organizaons will have
dierent structures, goals and personnel proles and will therefore priorize accordingly.
Drawing from the WHO/ILO model of Prevent, Promote, and Support, we ask individuals, managers, and
organizaons to take acon under each of these headings to posively aect organizaonal culture. These
acons will be laid out in Acon Plans developed by organizaons in accordance with their specic
condions and available resources. An example of an Acon Plan can be found in the Implementaon
Guide which accompanies this Scorecard.
Prevent
Promote
Support
1. Risk Assessment (Prevention
& mitigation)
3. Manager Training
7. Enabling Dignified Work
2. Policy & Practice
Mainstreaming
4. Stigma reduction activities
8. Access to psychosocial
support
5. Mental Health Literacy
training
9. Quality control for
psychosocial support
6.Implemention of well-being
initiatives
Cross cutting
10. Leadership
11. Reporting
12. Participation

15
Prevent
Indicator 1: Risk Assessment
Approaches Requirements
Meets Requirements
Exceeds Requirements
Current risk assessment
activities include a psycho-
social section.
A review of psycho-social
risks* has been undertaken*.
Current risk assessment activities
include a psycho-social section.
A review of psycho-social risks* has
been undertaken*.
_______________________________
Psycho-social risk assessment
mitigation action plan created and
implemented.
Current risk assessment activities
include a psycho-social section.
______________________________
A review of psycho-social risks* has
been undertaken*.
Psycho-social risk assessment
mitigation action plan created and
implemented.
_____________________________
Review and improvement process in
place for psycho-social risk mitigation.
_______________________________
Evaluation of risk mitigation
strategies included in managers
performance appraisals.
* Psycho-social risks include, workload management, work/ life harmony, job control, working hours, interpersonal relationships
** May be a pilot programme in one or more duty stations
Prevent
Indicator 2: Policy & Practice Mainstreaming
Approaches Requirements
Meets Requirements
Exceeds Requirements
Mental health and well-being
review of existing policies*
and practices related to people
management across the
employee lifespan**.
Mental health and well-being review
of existing policies* related to
people management across the
employee lifespan**.
______________________________
Based on the MH&WB review,
policies flagged related to people
management are edited, or
authored, to ensure inclusion of
MH&WB considerations.
Mental health and well-being review
of existing policies* related to people
management across the employee
lifespan**.
_______________________________
Based on the MH&WB review, policies
flagged related to people management
are edited, or authored, to ensure
inclusion of MH&WB considerations.
All policies related to people
management are regularly reviewed,
and accountability mechanisms are
implemented.
*Examples may include: the areas of pre and post deployment, recruitment, workload management, workforce planning, FWA, and
work-life harmony, RTW, Sick leave policy, reasonable accommodation, policy on mobility, prevention of harassment, OHS,
performance management, values and behaviour framework, People / HR strategy, diversity equity and inclusion, disability,
LGBTQI, Staff Safety and Security, etc.
** recruitment, on-boarding, re-assignment, retirement/termination

16
Promote
Indicator 3: Manager Education and Training
Approaches Requirements
Meets Requirements
Exceeds Requirements
Training* for new Managers on
workplace mental health and
wellbeing. is included in
induction.
Training* for new Managers on
workplace mental health and
wellbeing. is included in induction.
__________________________
Training* for all Managers on
workplace mental health and
wellbeing is integrated into
managers development and learning
initiatives
Managers have access to coaching
and guidance related to mental
health and well-being in the
workplace.
Training* for new Managers is
included in induction.
__________________________
Training* for all Managers on
workplace mental health and
wellbeing is integrated into
management development and
learning initiatives
Managers have access to coaching
and guidance related to mental
health and well-being in the
workplace.
Manager education and training
initiatives are evaluated, and results
are integrated to ensure continuous
improvement.
*Modify Lead & Learn (or similar courses) to organizational needs
Promote
Indicator 4: Stigma Reduction Activities
Approaches Requirements
Meets Requirements
Exceeds Requirements
Data is gathered to understand
stigma within the organization.
An inter-disciplinary well-being
working group is established to
agree appropriate evidence-based
actions
Data is gathered to understand
stigma within the organization.
An inter-disciplinary well-being
working group is established to
agree appropriate evidence-based
actions
Stigma reduction interventions,
informed by evidence-based
research and persons with lived
experience, are enacted.
Data is gathered to understand
stigma within the organization.
An inter-disciplinary well-being
working group is established to
agree appropriate evidence-based
actions
Stigma reduction interventions,
informed by evidence-based
research and persons with lived
experience, are enacted.
Stigma reduction campaign is
mainstreamed and/ data is
collected to measure impact.

17
Promote
Indicator 5: Mental Health Literacy
Approaches Requirements
Meets Requirements
Exceeds Requirements
MH literacy training is included in
onboarding learning programmes.
MH literacy training is included in
onboarding learning programmes.
MH literacy training is available for
all existing personnel in learning
programmes.
MH literacy training is included in
onboarding learning programmes.
MH literacy training is available for
all existing personnel in learning
programmes.
Targeted training (inc. suicide
prevention) for specific roles (HR,
Security, frontline workers) is
provided.
Promote
Indicator 6: Implementation of Well-being Initiatives
Approaches Requirements
Meets Requirements
Exceeds Requirements
Process for implementing evidence
informed well-being activities is
developed - (e.g., Inter-disciplinary
well-being* working group)
Process for implementing evidence
informed well-being activities is
developed - (e.g., Inter-disciplinary
well-being* working group)
Personnel can access evidence
informed training programmes and
well-being tools online.
Well-being initiatives are
accessible organization-wide.
Process for implementing evidence
informed well-being activities is
developed - (e.g., Inter-disciplinary
well-being* working group)
Staff can access evidence informed
training programmes and well-
being tools online.
Well-being initiatives are
accessible organization-wide.
Well-being initiatives are monitored
for uptake and utility and assessed
regularly.
*Well-being topics may include but are not limited to: Stress management, sleep hygiene, mindfulness, yoga, healthy
eating, etc.

18
Support
Indicator 7: Enabling Dignified Work (Reasonable Accommodation and Return to Work)
Approaches Requirements
Meets Requirements
Exceeds Requirements
Ad hoc implementation of
Reasonable Accommodation and
Return-to-Work.
Ad hoc implementation of
reasonable accommodations, and
Return-to-Work, without formal
guidelines.
Reasonable accommodation policy
exists and is implemented
consistently in a multi-
disciplinary approach.
Clients can provide feedback on
the practice and policy.
Ad hoc implementation of
reasonable accommodations, and
Return-to-Work.
Reasonable accommodation policy
exists and is implemented
consistently in a multi-
disciplinary approach.
Clients can provide feedback on
the practice and policy.
Case management provided for
personnel.
Support
Indicator 8: Access to Psychosocial Support
Approaches Requirements
Meets Requirements
Exceeds Requirements
Information available to all
personnel on support services in-
house and external.
___________________________
Assess/review current insurance
carriers for MH coverage.
Mapping of clients for insurance
coverage*
Information available to all
personnel on support services in-
house and external.
Assess/review current insurance
carriers for MH coverage. Mapping
of clients for insurance coverage*
From the onset of UN contract, all
personnel and dependents have
insurance coverage which
includes MH needs.
Support within 72 hours regardless
of duty station
Support in case of critical incident
and crisis management
____________________________
Support for conflict resolution
(reconciliation, conflict coaching,
mediation)
-Pre-deployment counseling
-Post-deployment counseling
Pro-active counseling support for
staff in unstable/ high risk
environment
Information available to all personnel
on support services in-house and
external.
Assess/review current insurance
carriers for MH coverage. Mapping of
clients for insurance coverage*
_____________________________
From the onset of UN contract, all
personnel and dependents have
insurance coverage which includes
MH needs.
_____________________________
Support within 72 hours regardless of
duty station
_____________________________
Support in case of critical incident
and crisis management
Support for conflict resolution
(reconciliation, conflict coaching,
mediation)
-Pre-deployment counseling
-Post-deployment counseling
Pro-active counseling support for
staff in unstable/ high risk environment

19
Family Liaison Officer available to
address the well-being needs of the
families of staff.
_______________________________
Ensure appropriate** insurance
coverage includes MH needs of all UN
personnel and dependents
*Including dependents & non-staff (long term consultants)
** Ensure reimbursement is client-friendly and an easy one-step process. Direct to recognized MH services without
prescription/referral.
Support
Indicator 9: Quality Control for Psychosocial Support
Approaches Requirements
Meets Requirements
Exceeds Requirements
Complete mapping of currently
available psychosocial services
(internal and external)
Establishment of lead for
psychosocial support with
responsibility for oversight of
psychosocial programme
Provide clinical supervision for
staff counselors
Complete mapping of currently
available psychosocial services
(internal and external)
Establishment of lead
psychosocial staff with responsibility
for oversight of psychosocial
programme
Provide clinical supervision for
staff counselors
Ensure providers are licensed/
accredited and those who are not
have a plan in place to achieve as
per UNSSCG Guidelines
Complete mapping of currently
available psychosocial services
(internal and external)
Establishment of lead
psychosocial staff with responsibility
for oversight of psychosocial
programme
__________________________
Provide clinical supervision for
staff counselors
Ensure providers are licensed/
accredited and those who are not
have a plan in place to achieve as
per UNSSCG Guidelines
Ensure a feedback mechanism
exists for client input and review.
Minimum of 20 hours yearly
continuing education available

20
Cross cutting
Indicator 10: Leadership
Approaches Requirements
Meets Requirements
Exceeds Requirements
Leadership focal point is assigned
to assume overall responsibility for
mental health programming.
____________________________
Leadership regularly*
communicates with staff about the
importance of MH&WB.
Leadership focal point is assigned
to assume overall responsibility for
mental health programming.
____________________________
Leadership regularly*
communicates with staff about the
importance of MH&WB.
Leadership assigns or assumes
responsibility for key actions in a
highly visible manner to
demonstrate action being taken.
Mental Health and Well-being***, is
included as an assessment criteria
of leaders’ performance.
Leadership focal point is assigned
to assume overall responsibility for
mental health programming.
____________________________
Leadership regularly*
communicates with staff about the
importance of MH&WB.
Leadership assigns or assumes
responsibility for key actions in a
highly visible manner to
demonstrate action being taken.
Mental Health and Well-being*** is
included as an assessment criteria
of leaders' performance. **
Leadership takes an active role in
securing funding for
implementation of the Mental Health
and Well-being Strategy.
*3 times or more per year
** This should include, recruitment criteria, performance planning and inclusion in 360 assessments. It should be
focused on the manager’s behavior in supporting good mental health and reducing psycho-social risks in the
workplace.
Cross cutting
Indicator 11: Reporting
Approaches Requirements
Meets Requirements
Exceeds Requirements
Organization takes part in UNHI
survey at minimum every two years.
Yearly completion of the MH&WB
Scorecard
Organization takes part in UNHI
survey minimum every two years.
Yearly completion of the MH&WB
Scorecard
MH&WB Action Plan created and
progress reported* to personnel.
Organization takes part in UNHI
survey minimum every two years.
Yearly completion of the MH&WB
Scorecard
MH&WB Action Plan created and
progress reported* to personnel.
* This includes a report of action taken, developed yearly and shared with staff

21
Cross cutting
Indicator 12: Participation
Approaches Requirements
Meets Requirements
Exceeds Requirements
All relevant mental health and well-
being committees, working groups,
and/or tasks forces seek
membership and/or input from
those with lived experience*.
All relevant mental health and well-
being committees, working groups,
and/or tasks forces seek
membership and/or input from
those with lived experience*.
Organization has either a
representative or focal point for
the Implementation Board
All relevant mental health and well-
being committees, working groups,
and/or tasks forces seek membership
and/or input from those with lived
experience*.
_______________________________
Organization has either a
representative or focal point for the
Implementation Board
Organization has dedicated
resources to the system wide
implementation effort either financially
or in-kind.
* Process for including the voices of personnel with a lived experience of poor mental health is established

22
Annex III:
PSYCHOSOCIAL RISKS
Examples of psychosocial risks at work and organizational interventions that employers can take to
address them
Aspect of work
Potenal psycho-social risks
Examples of organizaonal intervenons
Job content/ task design
Lack of variety in the work: under-use of
skills or under-skilled for work
- Parcipatory approaches to job design
- Task rotaon or job redesign
Workload and work pace
Heavy workloads, high work pace, high
me pressure, connual and short
deadlines, understang
- Limits on working hours or number of shis
- Achievable deadlines and targets
- Adequate job demands (neither too high or too
low)
- Safe stang levels
Work schedule
Long or unsocial work hours, shi
working, inexible hours
- Parcipatory approaches to scheduling
- Flexible working arrangements
- Planned breaks
- Welfare facilies and support available during
atypical hours
Job control
Lack of control over job design or
workload, limited parcipaon in
deciding one’s own work
- Parcipatory approaches to job design, work
organizaon and decision-making
- Frequent and open communicaon
Environment and
equipment
Unsafe equipment and resources, poor
physical working condions (such as
poor lighng, excessive or irritang
noise, poor ergonomics)
- Investment in improved environments and
equipment meeng health and safety
requirements, in consultaons with workers
and/or their representaves
Organizaonal culture
Unclear organizaonal objecves, poor
communicaon, culture that enables
discriminaon or abuse
- Opportunies for meaningful consultaon and
cooperaon with workers and/or their
representaves
- Organizaonal frameworks for dealing with
unfair treatment, oensive behaviour and abuse
- Support for aected workers, including access to
workers’ representaves – where they exist
Interpersonal
relaonships at work
Social or physical isolaon, limited
support from supervisors or colleagues,
authoritarian supervision and poor line
management, violence, harassment or
bullying, discriminaon and exclusion
- Frameworks for prevenng violence, harassment
and discriminaons, and for invesng and
dealing eecvely with incidents
- Opportunies to improve knowledge, atudes
and skills for supervisors and managers
- Opportunies for peer support, including in
atypical working hours or sites
Role in organizaon
Unclear job role within the organizaon
or team
- Clearly dened sustainable work roles, reporng
structures and performance requirements
Career development
Under- or over- promoon, job
insecurity, poor investment in
development, punive procedures for
sickness absence and performance
management
- Fair and good career training and retraining
prospects
- Formal, secure work through contracts in line
with naonal law and pracce, including paid
sick leave
- Equal opportunies and transparency in all
processes
- Supports performance management
Home-work interface
Conicng home/work demands, being
away from home for work
- Flexible working arrangements
- Support for careers

23
Annex IV:
JIU RECOMMENDATIONS WITH CORRESPONDING SCORECARD INDICATORS
Recommendaon 1
The execuve heads of those United Naons system organizaons that do not already parcipate on the
Implementaon Board of the United Naons System Mental Health and Well-being Strategy should
nominate a representave to serve on the Board by its rst meeng in 2024.
Indicator 12: Parcipaon
- Organizaon has either a representave or focal point for the Implementaon Board.
Recommendaon 2
Execuve heads of United Naons system organizaons, who have not already done so, should dene an
evidence-based and data-driven organizaonal approach to the mental health and well-being of their
personnel and design, by the end of 2025, a workplace acon plan and reect its principles in their
enterprise risk management process, their occupaonal health and safety framework and their human
resources strategies.
Indicator 1: Risk Migaon
- Psycho-social risk assessment migaon acon plan created and implemented.
Indicator 2: Policy and Pracce Mainstreaming
- All policies related to people management are regularly reviewed and accountability mechanisms
are implemented.
Recommendaon 3
Legislave and/or governing bodies of United Naons system organizaons should request that execuve
heads provide, by the end of 2026, an update on the development and implementaon of the mental
health and well-being workplace acon plan developed according to their evidence-based and data-driven
organizaonal approach on the maer.
Indicator 10: Leadership
- Leadership assigns or assumes responsibility for key acons in a highly visible manner to demonstrate
acon being taken.
Indicator 11: Reporng
- Mental Health and Well-being Acon Plan created and progress reported to personnel (and legislave
bodies).

24
Recommendaon 4
By the end of 2024, execuve heads of United Naons system organizaons should review the rules
governing the return to work of personnel, including provisions for granng accommodaons to facilitate
the return process, in order to ensure the inclusiveness of mental health-related consideraons, and
develop standard operang procedures that clearly idenfy roles and responsibilies, including decision-
making.
Indicator 7: Enabling Dignied Work
- Reasonable accommodaon policy exists and is implemented consistently in a mul-disciplinary
approach.
- Clients can provide feedback in the pracce and policy
Recommendaon 5
By the end of 2024, execuve heads of United Naons system organizaons should assess and idenfy any
gaps or areas to improve their counselling funcon in their organizaonal context, using the guidance on
professional standards for counsellors prepared by the United Naons Sta/Stress Counsellors Group and
endorsed by the Human Resources Network of the United Naons System Chief Execuves Board for
Coordinaon, as well as key elements highlighted by the Joint Inspecon Unit in the present report.
Indicator 9: Quality Control for Psychosocial Support
- Ensure providers are licensed/ accredited and those who are not have a plan in place to achieve as
per UNSSCG Guidelines
- Provide clinical supervision for sta counselors
- Minimum of 20 hours yearly connuing educaon available
Recommendaon 6
The Secretary-General should request the High-level Commiee on Management of the United Naons
System Chief Execuves Board for Coordinaon to explore and report on, by the end of 2024, opons to
ensure that a mental health praconer is posted to all countries with D- or E-category duty staons.
Indicator 8: Access to Psychosocial Support
- Informaon available to all personnel on support services in-house and external.
- Support within 72 hours regardless of duty staon
- Support in case of crical incident and crisis management
- Pro-acve counseling support for sta in unstable/ high risk environment
- Pre and Post -deployment counselling
Recommendaon 7
The General Assembly should consider, by its eigheth session, the conclusions of the High-level
Commiee on Management of the United Naons System Chief Execuves Board for Coordinaon
regarding resources to support the posng of a mental health praconer to countries with D- or E-
category duty staons.
25
Indicator 8: Psychosocial Access
- Informaon available to all personnel on support services in-house and external.
- Support within 72 hours regardless of duty staon
- Support in case of crical incident and crisis management
- Pro-acve counseling support for sta in unstable/ high risk environment
- Pre and Post -deployment counselling
Recommendaon 8
Execuve heads of United Naons system organizaons should ensure that their organizaons collaborate
on the mapping of psychosocial support capacity available in all locaons and consider the system-wide
capacity when designing their workplace acon plans, capitalizing on shared services, cost-sharing and
other models for cost-eecve and ecient delivery.
Indicator 9: Quality Control for Psychosocial Support
- Complete mapping of currently available psychosocial services (internal and external)
- Establishment of lead psychosocial sta with responsibility for oversight of psychosocial program
Recommendaon 9
Execuve heads of United Naons system organizaons should ensure that their workplace acon plans
on the mental health and well-being of their personnel, to be designed by the end of 2025, idenfy barriers
to accessing psychosocial support services, including priorizing sgma reducon through mental health
literacy iniaves, outreach and health-promoon measures.
Indicator 4: Mental Health Literacy
- Mental health literacy is available for all personnel in learning programs
- Specialized training exists for managers
Indicator 5: Sgma Reducon
- Sgma reducon intervenons, informed by evidence-based research and persons with lived
experience, are enacted.
- Sgma reducon campaign is mainstreamed and/or index/surveys created to measure impact.
Recommendaon 10
To maximize return on investment, execuve heads of United Naons system organizaons should, by
2026, ensure that well-being programmes and acvies are embedded in and complement the evidence-
based and data-driven approach of the organizaon to mental health and well-being and are rounely
monitored and assessed.
26
Indicator 6: Well-being Iniaves
- Process for implemenng evidence informed well-being acvies is developed
- Sta can access evidence informed training programs and well-being tools online.
- Well-being iniaves are monitored for uptake and ulity and assessed regularly.
Indicator 11: Reporng
- Organizaon takes part in UNHI survey minimum every two years.
- MH&WB Acon Plan created and progress reported* to personnel.
- Yearly compleon of the MH&WB Scorecard
Recommendaon 11
Execuve heads of United Naons system organizaons should explore integrang, by the end of 2024,
mental health and well-being consideraons into training programmes, in parcular for managers, as a
means to provide opportunies for facilitated discussions and enhanced learning and to support
employees with mental health condions.
Indicator 3: Manager Educaon and Training
- Training* for all Managers on workplace mental health and wellbeing is integrated into managers
development and learning iniaves

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
0
BACKGROUND
The implementation of the 2018-23 Mental Health and Well-being Strategy demonstrated that there are many benets
of a system-wide approach. The recently published JIU Review ‘mental health and well-being policies and practices in
the United Nations system organizations’ clearly outlines the negative nancial impacts of poor mental health at the
UN and the organizational risks posed by not taking a system wide approach.
Benets of a system-wide approach, with resources for global co-ordination include:
• effective use of resources to minimize duplication
• standardized reporting and actions
• sharing of good practices
• development of tools and learning products that can be adapted by UN Organizations to reduce resources
required to develop these individually
• systemwide communication efforts, including campaigns, website, and events
From 2018 through 2023 the implementation of the Strategy was supported by voluntary contributions from
participating organizations. This approach has proven to lack funding predictability which in turn has made an impact
on the overall sustainability of the current Strategy implementation. A budget envelope is required to ensure continuity
in delivery and sustained support to system-wide Strategy implementation.
This Appendix contains the details of the resource proposal of the next iteration of the Strategy.

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
1
PROPOSED STAFFING STRUCTURE
P5 – Global Lead (full time)
Reports to: Chair of the Implementation Board.
Overall Purpose: Leading the System wide Strategy Implementation.
Main responsibilities:
▪ Provide strategic leadership and advocacy for decision makers to implement the Strategy across the UN System.
▪ Provide guidance to UN organizations on how to implement the Strategy.
▪ Ensure integration of the Strategy with other system-wide strategies
▪ Lead programmes of work as agreed with the Implementation Board.
▪ Lead the development of policies, tools and learning products that can be adapted by UN Organizations to share
resources required to develop products and programmes individually.
▪ Undertake communication and change management activities, including campaigns, multimedia and digital
products and events.
▪ Maintain strategic partnerships within and outside of the UN System.
▪ Oversee and ensure a streamlined monitoring, evaluation and reporting.
▪ Manage the budget and funds received.
▪ Manage personnel employed or seconded to support strategy implementation.
▪ Manage the recruitment of staff and consultants.
P3 – Programme Manager (Mental Health)– Monitoring & Evaluation/Data Analyst (full time)
Reports to: Global Lead.
Overall purpose: Monitoring and evaluation, analysing data, reporting and providing technical input.
Main responsibilities:
▪ Provide technical input in activities concerning mental health data, mental health promotion, prevention of
mental health conditions, and mental health care.
▪ Provide technical input in the development, implementation and evaluation of projects emanating from the
Strategy.
▪ Coordinate data collection and analyse the data collected.
▪ Co-ordinate the implementation the Strategy Scorecards, including data management, report writing and drafting
recommendations.
▪ Prepare reports as required for HRN, HLCM and other stakeholders.
G6 – Administrative Assistant (full time)
Reports to: Global Lead.
Overall purpose: Providing administrative support to the team and Implementation Board.
Main responsibilities:
• Perform administrative duties, as required (e.g., operational travel programme; monitoring accounts and
payment to vendors and individual contractors for services; physical space planning; identification of team’s
technology needs and maintenance of equipment, software and systems; scheduling, organizing and
coordinating meetings, workshops and retreats).
• Draft routine correspondence, monitor team inbox and maintains the shared SharePoint site.
• Assist with the collection and analysis of data as well as preparation of data presentations and reports for
information sharing, responding to queries, knowledge management, planning and decision making.

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
2
• Assist with visualizations and updating information material.
• Provide support and manage administrative elements of the recruitment of staff and consultants.
• Assist in the preparation of yearly budgets, monitors expenditures and compares with approved budget
• Assist with day-to-day administration of contracts between the UN and external contractors for outsourced
services, audits invoices and processes payments.
P5 – UN Secretariat – 20% in 2024
Reports to: Chair of the Implementation Board.
Overall Purpose: Working as the Secretariat to the Implementation Board and in Leading the System wide Strategy
Implementation during the transition.
Main responsibilities:
• Cover Global Lead functions until Global Lead is recruited (estimated 1 March 2024) and transitioned in 2024.
• Cover Global Lead functions during leave.
• Work as the Secretariat of the Implementation Board.
PROPOSED NON-STAFF
Consultants
Overall purpose: Consultants will be engaged to support implementation of the Strategy, reporting to the global lead.
The consultants will be developing products, tools, resources, material, project and activities, allowing participating
organization to not have to reinvent the wheel. Key outputs:
• Develop learning products, tools and training resources - including project management and translation
• Develop communication and engagement related material, activities (events, speakers, etc) – including
project management and translation
• Contribute to policy reviews

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
3
PROPOSED STAFFING LOCATION OPTIONS
(in alphabetical order)
Bonn
The advantage of choosing Bonn is that it is a well-connected and accessible city and has a similar cost range
compared to least expensive location. In addition, placing the team in Bonn would support the strategic value of OneHR
which also is in Bonn. The presence of the UN Staff College is an added benet.
The disadvantage of Bonn is that it would be the headquarters for UN System organizations representing the lowest
headcount in relation to the three locations being considered.
Geneva
In contrast to Bonn, Geneva’s advantage is that it is the duty station with the highest number of UN System
organizations, representing the highest headcount in relation to the three locations being considered. The headquarters
of many Agencies, Funds and Programmes (AFPs) are in Geneva and there is increased access to senior-level decision
authorities. The location is also well-connected and accessible.
The disadvantage of Geneva is that it is the costliest option under consideration.
Vienna
The advantage of Vienna is that it is the least costly option, while still being well-connected and accessible.
The disadvantage of Vienna is that it has a lower number of UN System organizations, when comparing it to Geneva.
At a meeting of Mental Health and Well-being Strategy Implementation Board held on 13 September 2023 most
organizations present favoured Geneva as the rst option.

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
4
PROPOSED 2024 Budget
Table I below provides the proposed budget for staff and non-staff costs for the three location options.
Table I:
Proposed 2024 Budget
Location Options
Bonn
Geneva
Vienna
Staff Cost (including ASHI)
1 P5 Global Lead
(Full time, 2024 10 months)
$ 196,833
$ 215,667
$ 184,500
1 P3 Programme Manager (Mental Health)–
Monitoring & Evaluation / Data Analyst
(Full time, 2024 10 months)
$ 151,750
$ 162,083
$ 139,750
1 G6 Administrative Assistant
(Full time, 2024 10 months)
$ 71,667
$ 124,167
$ 80,167
1 P5 NY
( Part-time, 2024 20%)
$ 47,240
$ 47,240
$ 47,240
Subtotal
$ 467,490
$ 549,157
$ 451,657
Non-Staff Cost
Consultants:
a) Develop learning products, tools and training
resources (including project management and
translation)
b) Develop communication and engagement
related material, activities (events, speakers, etc.)
c) Contribute to policy reviews (including
translation)
$ 190,000
$ 190,000
$ 190,000
Website (including translation)
$ 60,000
$ 60,000
$ 60,000
Travel
1
2
3
$ 15,735
$ 20,140
$ 18,443
Common Premises Services Cost
$ 20,625
$ 31,500
$ 27,900
Staff Development
$ 10,000
$ 10,000
$ 10,000
ICT and Office Supplies
$ 5,000
$ 5,000
$ 5,000
Subtotal
$ 301,360
$ 316,640
$ 311,343
Total
$ 768,850
$ 865,797
$ 763,000
1
Cologne/Frankfurt to/from: Bern, Copenhagen, Geneva (2), London, Madrid, Montreal, Nairobi, New York, Paris, Rome and Vienna
2
Geneva to/from: Bern, Bonn, Copenhagen, London, Madrid, Montreal, Nairobi, New York, Paris, Rome and Vienna
3
Vienna to/from: Bern, Bonn, Copenhagen, Geneva (2) London, Madrid, Montreal, Nairobi, New York, Paris and Rome.

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
5
PROPOSED COST-SHARING DISTRIBUTION MODEL
It is proposed that the budget is cost-shared by all CEB/HLCM/HRN member organizations. The proposal is that the
share for each CEB/HLCM/HRN member organizations be based on:
a) its size as per the CEB Global Headcount as of 31 December 2022 for central activities;
b) a maximum of US$ 70,000 for organizations with a headcount of more than 25,000 except the UN Secretariat
which will have a higher share; and
c) a minimum of US$ 5,000 for organization with a headcount of or less than 500.
The above approach results in the cost sharing and billable amounts for 2024 as reflected in Table II.

Appendix 2:
Mental Health and Well-being Strategy
Proposed Staffing Structure, Location Options, 2024 Budget
and Cost-Sharing Distribution Model
6
Table II:
Indicative distribution options of the 2024 budget among participating organizations
Acronym
Organization(s)
Headcount end
2022
Proposed Contribution 2024
CEB MEMBERS
Maximum
Minimum
UN
United Nations
New York
46,045
$ 80,000
$ 75,000
UNDP
United Nations Development Programme
New York
29,077
$ 70,000
$ 62,500
WB
World Bank
Washington
25,119
$ 70,000
$ 62,500
WFP
World Food Programme
Rome
22,984
$ 60,000
$ 55,000
UNICEF
United Nations Children's Fund
New York
22,522
$ 60,000
$ 55,000
UNHCR
United Nations High Commissioner for Refugees
Geneva
20,787
$ 60,000
$ 55,000
IOM
International Organization for Migration
Geneva
20,715
$ 60,000
$ 55,000
WHO
World Health Organization
Geneva
18,141
$ 55,000
$ 47,500
FAO
Food and Agriculture Organization
Rome
13,065
$ 46,000
$ 41,000
IMF
International Monetary Fund
Washington
5,471
$ 30,000
$ 25,000
UNOPS
United Nations Office for Project Services
Copenhagen
5,314
$ 30,000
$ 25,000
UNFPA
United Nations Population Fund
New York
5,038
$ 30,000
$ 25,000
ILO
International Labour Organization
Geneva
4,881
$ 24,000
$ 19,000
UNESCO
United Nations Educational, Scientific and Cultural
Organization
Paris
4,725
$ 24,000
$ 19,000
UN Women
United Nations Women
New York
2,937
$ 14,000
$ 12,500
IAEA
International Atomic Energy Agency
Vienna
2,745
$ 14,000
$ 12,500
UNIDO
United Nations Industrial Development Organization
Vienna
1,624
$ 14,000
$ 12,500
WIPO
World Intellectual Property Organization
Geneva
1,360
$ 14,000
$ 12,500
IFAD
International Fund for Agricultural Development
Rome
1,172
$ 14,000
$ 12,500
ICAO
International Civil Aviation Organization
Montreal
973
$ 10,000
$ 8,000
ITU
International Telecommunication Union
Geneva
829
$ 10,000
$ 8,000
WTO
World Trade Organization
Geneva
620
$ 10,000
$ 8,000
WMO
World Meteorological Organization
Geneva
344
$ 5,000
$ 4,000
IMO
International Maritime Organization
London
326
$ 5,000
$ 4,000
UNRWA
United Nations Relief and Works Agency
Amman
314
$ 5,000
$ 4,000
UPU
Universal Postal Union
Bern
264
$ 5,000
$ 4,000
UNWTO
United Nations World Tourism Organization
Madrid
196
$ 5,000
$ 4,000
HRN MEMBERS
PAHO
Pan American Health Organization
Washington
1,827
$ 14,000
$ 12,500
ITC
International Trade Centre
Geneva
1,049
$ 14,000
$ 12,500
UNAIDS
Joint United Nations Programme on HIV/AIDS
Geneva
759
$ 10,000
$ 8,000
UNFCCC
United Nations Framework Convention on Climate
Change
Bonn
366
$ 5,000
$ 4,000
Total
261,589
$ 867,000
$ 765,000
