
New Tricks for an Old Measure: The Development of the Barratt
Impulsiveness Scale–Brief (BIS-Brief)
Lynne Steinberg and Carla Sharp
University of Houston
Matthew S. Stanford
Baylor University
Andra Teten Tharp
Centers for Disease Control and Prevention, Atlanta, Georgia
The Barratt Impulsivity Scale (BIS), a 30-item self-report measure, is one of the most commonly used
scales for the assessment of the personality construct of impulsiveness. It has recently marked 50 years
of use in research and clinical settings. The current BIS-11 is held to measure 3 theoretical subtraits,
namely, attentional, motor, and non-planning impulsiveness. We evaluated the factor structure of the BIS
using full information item bifactor analysis for Likert-type items. We found no evidence supporting the
3-factor model. In fact, half of the items do not share any relation with other items and do not form any
factor. In light of this, we introduce a unidimensional Barratt Impulsiveness Scale–Brief (BIS-Brief) that
includes 8 of the original BIS-11 items. Next, we present evidence of construct validity comparing scores
obtained with the BIS-Brief against the original BIS total scores using data from (a) a community sample
of borderline personality patients and normal controls, (b) a forensic sample, and (c) an inpatient sample
of young adults and adolescents. We demonstrated similar indices of construct validity that is observed
for the BIS-11 total score with the BIS-Brief score. Use of the BIS-Brief in clinical assessment settings
and large epidemiological studies of psychiatric disorders will reduce the burden on respondents without
loss of information.
Keywords: Barratt Impulsiveness Scale, item response theory, assessment
The construct of impulsiveness is broadly defined as “a predis-
position toward rapid, unplanned reactions to internal or external
stimuli without regard to the negative consequences of these
reactions to the impulsive individuals or to others” (Moeller,
Barratt, Dougherty, Schmitz, & Swann, 2001, p. 1784). Impulsive-
ness has been a focus of great interest both in the personality and
clinical psychology literature due to its relevance for occupational
and educational outcomes, as well as a wide range of psychiatric
disorders, including substance use disorders (de Wit, 2009), anti-
social behavior (Barratt, Stanford, Kent, & Felthous, 1997), bor-
derline personality disorder (BPD; Links, Heslegrave, & van Ree-
kum, 1999), intermittent explosive disorder (Brady, Myrick, &
McElroy, 1998), pathological gambling (Blaszczynski & Nower,
2002), bipolar disorder (Swann, Steinberg, Lijffijt, & Moeller,
2008), attention-deficit/hyperactivity disorder, and conduct prob-
lems in children (Nigg, 2003).
One of the most well-known and most used measures of impul-
siveness is the Barratt Impulsiveness Scale (BIS; Barratt, 1959).
The BIS, currently in its 11th revision (Patton, Stanford, & Barratt,
1995), is a 30-item self-report instrument designed to assess the
personality/behavioral construct of impulsiveness. In 2009, the
BIS celebrated its 50th anniversary, and by March 2009, 551
citations of the BIS-11 were recorded (Stanford et al., 2009),
building on the large number of publications using the preceding
versions of the instrument.
Given its widespread use, the BIS has been highly influential for
contemporary conceptualizations of impulsivity in personality and
clinical literature. Like many personality constructs, there has been
disagreement about the exact number of subtraits of impulsiveness,
ranging from two (Reynolds, Ortengren, Richards, & de Wit,
2006) to as many as five subtraits (Meda et al., 2009). Barratt’s
conceptualization of impulsiveness as described in the BIS
(Version 10) includes the theoretical subtraits of Cognitive Impul-
siveness, Motor Impulsiveness, and Non-Planning Impulsiveness
(Barratt, 1985). More recently, Patton et al. (1995) conducted a
second-order factor analysis and demonstrated the three-
component trait structure. Within this three-component conceptu-
alization, Cognitive Impulsiveness refers to the tendency to make
quick decisions, Motor Impulsiveness refers to a tendency to act
without thinking, and Non-Planning Impulsiveness refers to a lack
of “futuring” or forethought (Barratt, 1985). This conceptualiza-
tion of impulsiveness is in line with most empirical research to
date (Lejeuz, Magisdson, Mitchell, Stevens, & de Wit, 2010),
which have consistently conceptualized impulsiveness to include
This article was published Online First November 12, 2012.
Lynne Steinberg and Carla Sharp, Department of Psychology, Univer-
sity of Houston; Matthew S. Stanford, Department of Psychology and
Neuroscience, Baylor University; Andra Teten Tharp, Centers for Disease
Control and Prevention, Atlanta, Georgia.
The findings and conclusions in this article are those of the authors and
do not necessarily represent the official position of the Centers for Disease
Control and Prevention.
Correspondence concerning this article should be addressed to Lynne
Steinberg, Department of Psychology, 126 Heyne Building, University of
Psychological Assessment © 2012 American Psychological Association
2013, Vol. 25, No. 1, 216 –226 1040-3590/13/$12.00 DOI: 10.1037/a0030550
216
diminished ability to focus on tasks (i.e., attentional impulsive-
ness) and/or persist in tasks (i.e., motor impulsiveness); a tendency
to act on the spur of the moment and poor future planning (i.e.,
non-planning impulsiveness; Patton et al., 1995; Whiteside &
Lynam, 2001); diminished ability to delay gratification or height-
ened discounting of reward as a function of delay as well as hypo-
and hypersensitivity to reward and punishment (Ainslie, 1975;
Gray, 1987); poor response inhibition and increased passive avoid-
ance (Logan, 1994); and diminished ability to regulate emotion,
sometimes referred to as “urgency” (Whiteside & Lynam, 2001).
Despite the above support for Barratt’s three-factor model, the
factor structure of the BIS was determined decades ago using
traditional factor analysis. Few studies since the original validation
of the BIS-11 have explicitly examined its factor structure and
psychometric properties. For example, Spinella (2007) conducted
a principal-component factor analysis with orthogonal rotation and
selected five items with the highest loadings on each of the three
established factors resulting in a 15-item version. Ireland and
Archer (2008) performed both confirmatory and principal-
component factor analysis to evaluate the factor structure of the
BIS-11. As was the case for the earlier factor analytic studies, the
analyses done in these studies used Pearson correlations, which
can result in spurious factors arising from differences in endorse-
ment of item response categories (often named “difficulty” factors
in educational measurement). However, to our knowledge, no
studies to date have examined the factor structure and individual
item performance of the BIS using current full information ap-
proaches appropriate for categorical item responses.
Against this background, the first aim of the present study was
to examine the established three-factor structure of the BIS
through a confirmatory multidimensional item response theory
(IRT) approach. Past research (e.g., Gibbons et al., 2008) suggests
that IRT item analysis of lengthy measures results in a reduction of
the number of items via a selection of items with optimal charac-
teristics; reliability may be even increased using fewer items (e.g.,
Steinberg & Thissen, 1996). This is advantageous for the use of the
BIS in large-scale epidemiological studies of psychiatric disorders
and for reducing the burden on respondents in clinical assessment
settings. In anticipation of the shortening of the BIS, our second
aim was to evaluate the construct validity of the new shorter BIS
by examining its performance against the original 30-item BIS-11
version in three samples: (a) an adult community sample of indi-
viduals meeting criteria for BPD and normal controls (King-Casas
et al., 2008; Patel, Sharp, & Fonagy, 2011), (b) an adult sample of
individuals who have engaged in domestic violence (Stanford,
Houston, & Baldridge, 2008), and (c) an adolescent and young
adult inpatient sample (Sharp, Ha, & Fonagy, 2011). We organize
the above two aims in two studies. Study 1 is an IRT study of the
BIS to examine its factor structure and item parameters, and Study
2 is a construct validity study of the shortened BIS.
Study 1: Measurement Models
The methods of IRT were used to evaluate the factor structure of
the 30-item BIS-11. The IRT model fitting and the computation of
the test statistics were performed using a beta version of IRTPRO
(Cai, du Toit, & Thissen, 2011; Thissen, 2009). Goodness of fit of
the IRT models was evaluated using the M
2
statistics and its
associated root-mean-square error of approximation (RMSEA)
value (Cai, Maydeu-Olivares, Coffman, & Thissen, 2006;
Maydeu-Olivares & Joe, 2005; Maydeu-Olivares & Joe, 2006;
Thissen, 2009), and the standardized local dependence (LD) chi-
square statistics (based on the LD statistic proposed by Chen &
Thissen, 1997). The graded response model (Samejima, 1969,
1997) was selected as the item response model for these analyses;
the graded model has often been found useful for questionnaire
data collected using Likert-type scales (for examples, see Fraley,
Waller, & Brennan, 2000; Gray-Little, Williams, & Hancock,
1997; Steinberg, 1994; Steinberg, 2001; Steinberg & Thissen,
1996).
Method
Participants. Undergraduate students at a midsized private
Southern university (N ⫽ 1,178; female 77.4%, male 22.6%; mean
age ⫽ 19.4, SD ⫽ 1.1; classification: freshman ⫽ 46.1%, sopho-
more ⫽ 23.5%, junior ⫽ 14.9%, and senior ⫽ 15.4%) were
recruited via a departmental research website accessible by all
undergraduate psychology majors. Among participants, 61.2%
were Caucasian, 12.8% were Hispanic, 12.8% were Asian/Pacific
Islander, 8.8% were African American, and 4.4% self-identified as
“other” or were multiracial. Students were given extra credit in a
course for completion of the BIS-11. These data were collected
with Institutional Review Board (IRB) approval.
Measures
The BIS-11 (Patton et al., 1995; Stanford et al., 2009). The
BIS-11 is a 30-item self-report measure designed to assess general
impulsiveness. The items are scored on a 4-point scale (1 ⫽
rarely/never,2⫽ occasionally,3⫽ often,4⫽ almost always/
always). Published reliability coefficients for the BIS-11 total
score (Cronbach’s ␣) range from 0.72 to 0.83.
Results
Evaluating the factor structure of the 30-item BIS-11.
Multidimensional model. Patton et al. (1995) investigated the
factor structure of the BIS-11 using principal components of
Pearson correlations with oblique rotation. Their analysis included
a second-order factor structure with three second-order factors that
were labeled attentional, non-planning, and motor impulsiveness.
Stanford et al. (2009) noted increased interest in the usefulness of
these subscales to explore relationships of impulsiveness with
other clinical symptoms. Our first analysis evaluating the factor
structure of the BIS-11 is designed to mirror the Patton et al.
structure using contemporary methods of full information bifactor
analysis.
Item bifactor analysis refers to a type of confirmatory multidi-
mensional IRT model in which one general factor and one or more
specific factors are specified (Cai, Yang, & Hansen, 2011). A
second-order factor is a constrained bifactor model (Yung,
McLeod, & Thissen, 1999); the second-order factor model adds
proportionality constraints within items across factors (Thissen &
Steinberg, 2010). Table 1 presents the IRT slope parameters and
standard errors for the full information item bifactor model. In this
analysis, one general factor (all 30 items) and three specific factors
(Attentional, Non-planning, and Motor Impulsiveness subscales)
217
BARRATT IMPULSIVENESS SCALE–BRIEF

are modeled. In IRT, slope parameters are algebraically related to
factor loadings and represent the degree of relation to the under-
lying construct; slopes that are 1 or greater are considered sub-
stantial. The column labeled a
1
is the general factor that includes
all 30 items. The columns a
2
, a
3
, and a
4
include the items for
attentional, motor, and non-planning impulsiveness as described in
Patton et al., respectively. (Note, the column labeled a lists the
slope parameters for a subsequent analysis that is described later.)
A perusal of the column for the general factor (a
1
) shows that only
about half of the items have substantial slope parameters. For
example, Item 19 “I act on the spur of the moment” has a
substantial slope parameter of 1.89; Item 15 “I like to think about
complex problems” has a low slope parameter of 0.47. This pattern
of item parameters implies that the responses to about half of the
items are not strongly related to what the general impulsiveness
factor measures.
The specific factors, a
2
–a
4
, reveal a different pattern of item
slope parameters. Each specific factor represents what has been
termed a “doublet” in the psychological measurement literature
and can be described as LD. LD occurs when items are more
strongly correlated than can be accounted for by the underlying
construct; in fact, the correlation may not represent a construct
intended to be measured by the item set. For example, the two
items comprising the content of a
2
, attentional impulsiveness, Item
28 “I am restless at the theater or lectures” and Item 11 “I ‘squirm’
at plays or lectures,” are similar in wording and meaning. The LD
is most likely a result of item similarity. These two items are the
only ones to show substantial slope parameters on that specific
factor; thus, this is not the attention construct intended for mea-
surement with the eight-item set, but rather excess covariation that
cannot be accounted for by the general factor. Similarly, the
specific factor “motor” impulsiveness (a
3
) is defined by LD be
-
tween the items, “I act on the spur of the moment” and “I act on
impulse”; the specific factor “non-planning” impulsiveness (a
4
)is
defined by LD between “I get easily bored when solving thought
problems” and “I like to think about complex problems.”
Table 1
Slope Parameter Estimates and Standard Errors for the Bifactor and Unidimensional IRT Models
Bifactor model
Unidimensional
model
Item Content a
1
SE a
2
SE a
3
SE a
4
SE a SE
11 I “squirm” at plays or lectures. 1.00 0.17 3.41 0.40 0.0 — 0.0 — 0.73 0.07
28 I am restless at the theater or
lectures.
1.02 0.15 2.99 0.29 0.0 — 0.0 — 0.78 0.07
6 I have “racing” thoughts. 0.43 0.06 0.57 0.07 0.0 — 0.0 — 0.60 0.06
5 I don’t pay attention. 1.12 0.08 0.56 0.07 0.0 — 0.0 — 1.20 0.08
9 I concentrate easily. 1.63 0.10 0.51 0.08 0.0 — 0.0 — 1.52 0.09
26 I often have extraneous thoughts
when thinking.
0.31 0.06 0.49 0.07 0.0 — 0.0 — 0.46 0.06
24 I change hobbies. 0.36 0.06 0.40 0.07 0.0 — 0.0 — 0.50 0.06
20 I am a steady thinker. 1.77 0.11 0.09 0.08 0.0 — 0.0 — 1.55 0.10
19 I act on the spur of the moment. 1.89 0.23 0.0 — 3.10 0.41 0.0 — 1.37 0.09
17 I act “on impulse.” 1.79 0.16 0.0 — 2.50 0.23 0.0 — 1.47 0.09
2 I do things without thinking. 1.33 0.09 0.0 — 0.81 0.09 0.0 — 1.45 0.09
3 I make up my mind quickly. ⫺0.14 0.06 0.0 — 0.66 0.08 0.0 — 0.05 0.06
4 I am happy-go-lucky. ⫺0.00 0.06 0.0 — 0.54 0.07 0.0 — 0.11 0.06
22 I buy things on impulse. 0.78 0.07 0.0 — 0.53 0.07 0.0 — 0.92 0.07
16 I change jobs. 0.25 0.07 0.0 — 0.36 0.08 0.0 — 0.38 0.07
21 I change residences. 0.13 0.06 0.0 — 0.15 0.07 0.0 — 0.20 0.06
25 I spend or charge more than I
earn.
0.77 0.07 0.0 — 0.13 0.07 0.0 — 0.80 0.07
30 I am future oriented. 0.85 0.07 0.0 — ⫺0.08 0.07 0.0 — 0.74 0.07
23 I can only think of one thing at a
time.
0.15 0.06 0.0 — ⫺0.21 0.07 0.0 — 0.13 0.06
18 I get easily bored when solving
thought problems.
1.09 0.15 0.0 — 0.0 — 1.52 0.22 0.79 0.07
15 I like to think about complex
problems.
0.76 0.08 0.0 — 0.0 — 1.11 0.19 0.47 0.06
29 I like puzzles. 0.45 0.07 0.0 — 0.0 — 0.72 0.10 0.32 0.06
12 I am a careful thinker. 1.87 0.11 0.0 — 0.0 — 0.14 0.13 1.59 0.10
27 I am more interested in the present
than the future.
0.39 0.06 0.0 — 0.0 — 0.04 0.08 0.45 0.06
14 I say things without thinking. 0.91 0.07 0.0 — 0.0 — ⫺0.02 0.09 1.11 0.08
10 I save regularly. 0.97 0.07 0.0 — 0.0 — ⫺0.12 0.09 0.89 0.07
13 I plan for job security. 1.11 0.08 0.0 — 0.0 — ⫺0.30 0.10 0.95 0.07
8 I am self-controlled. 1.42 0.09 0.0 — 0.0 — ⫺0.34 0.10 1.25 0.08
7 I plan trips well ahead of time. 1.23 0.09 0.0 — 0.0 — ⫺0.54 0.13 1.06 0.07
1 I plan tasks carefully. 1.67 0.11 0.0 — 0.0 — ⫺0.59 0.16 1.38 0.09
Note. IRT ⫽ item response theory. Boldface values indicate slope parameter values of 0.9 or higher. Dashes indicate that there are no standard errors for
fixed parameters.
218
STEINBERG, SHARP, STANFORD, AND THARP

The analysis using the bifactor model shows 14 additional pairs
of items with substantial LD (values 10 or greater are considered
noteworthy). The standardized LD chi-square statistics imply that
the bifactor model is not adequate to account for the excess
covariation between these item pairs.
The full information bifactor factor analysis conducted to eval-
uate the Patton et al. (1995) structure of the 30-item BIS-11
indicated that the pattern of item covariation is multidimensional.
However, the pattern of the slope parameters for the specific
factors shows a type of multidimensionality reflective of consis-
tency among item responses that is more LD than reflective of
individual differences on the intended constructs.
Unidimensional models. Because the bifactor model showed
that more than half of the items did not have a substantial relation
to the general underlying construct and that many of the items
show LD, we now aim to develop a shorter unidimensional version
of the BIS. The next IRT analysis takes a step back and investi-
gates the magnitude of the item slope parameters specifying a
unidimensional model. The motivation for this analysis is to select
the items that show substantial slope parameters for possible
inclusion in the brief BIS instrument. The two rightmost columns
of Table 1 lists the slope parameters and their associated standard
errors for the 30 BIS-11 items for the unidimensional model.
Again, more than half of the items do not show a substantial
relation to the underlying construct, and there are 19 pairs of items
that show LD; the standardized chi-square values range from 10 to
161. The substantial LD values indicate that a unidimensional
model is not adequate to account for the item covariation. Next, we
evaluated a unidimensional model that includes the 13 of the
BIS-11 items that showed substantial slope parameters in the
30-item unidimensional model analysis.
The graded model item parameters are presented in Table 2. The
slope parameters, representing the degree of relation of the item
response to the underlying construct as defined by the 13 BIS
items, shows substantial slopes for all items except Item 22 (“I buy
things on impulse”). However, four item pairs exhibit substantial
LD (the standardized chi-square values are 10.6, 12.4, 12.7, and
68.4). At this stage of the development of the brief version of the
BIS, we selected one item of the item pair 17 and 19 that exhibited
the largest LD index for omission (Item 17, “I act on impulse”).
With such a small item set, we focused on item content in addition
to item parameters to guide item selection. We omitted four
additional items for the following reasons: (a) Item 22 (“I buy
things on impulse”) has a low slope parameter, (b) Items 20 (“I am
a steady thinker”) and 13 (“I plan for job security”) may now have
different meaning today than when these items were written in the
1960s (e.g., the meaning of “steady thinker” is not clear, planning
for job security in the present global economy may not be possi-
ble), and (c) Item 7 (“I plan trips well ahead of time”) assumes the
respondent takes trips.
Development of the BIS-Brief. Our focus at this stage is to
evaluate the remaining eight items for inclusion in the new BIS-
Brief instrument. We are interested in developing a unidimensional
impulsiveness measure with items that have substantial slope
parameters and an adequate range of threshold parameters. Table
3 presents the slope and threshold parameter estimates for the eight
items. The graded IRT model showed satisfactory fit, M
2
(244) ⫽
706.12, p ⬍ .001; RMSEA ⫽ 0.04; however, there was one
noteworthy LD index for the item pair “I don’t pay attention” and
“I concentrate easily” (standardized
2
LD index ⫽ 10.4). An
analysis was done to evaluate the significance of the LD. Specif-
ically, a bifactor model that includes an equal-slope second factor
composed of the item pair (Items 5 and 9) that showed LD was
used. The estimated slope parameter for the specific factor is 1.14
with a standard error of 0.13. To evaluate the significance of the
LD, a likelihood ratio chi-square goodness-of-fit difference test
was used. The –2 log-likelihood obtained in the bifactor analysis
was subtracted from the –2 log-likelihood obtained in the eight-
item unidimensional analysis. The result is G
2
(1) ⫽ 12.5, p ⬍
.001. In practice, possible ways to deal with significant LD include
either (a) omitting one of the items in the pair or (b) forming a
testlet (Steinberg & Thissen, 1996; Thissen & Steinberg, 2010)of
the item pair by summing the item responses, thereby creating a
single “super” item. The testlet is then used for item parameter
estimation (so that the slope parameters are not influenced by the
excess covariation between the two items showing LD).
We opted for inclusion of the six items and the testlet compris-
ing Items 5 and 9 so that all eight items can be retained for the new
BIS-Brief measure. Table 4 lists the item parameters for the now
seven-item analysis (six items, one testlet). Because the testlet is
made from the sum of the two items, total scores can be calculated
by summing up the responses to the eight items. Thus, the testlet
Table 2
Graded Model Item Parameter Estimates for 13 BIS-11 Items
Item Brief content aSE b
1
SE b
2
SE b
3
SE
1 Plan tasks 1.55 0.10 ⫺1.01 0.07 0.58 0.06 2.75 0.15
2 Do things 1.57 0.10 ⫺0.67 0.06 1.58 0.09 3.23 0.20
5 Don’t pay attention 1.07 0.08 ⫺0.87 0.09 1.73 0.12 3.78 0.28
7 Plan trips 1.15 0.08 ⫺1.06 0.09 0.54 0.07 2.21 0.14
8 Self-controlled 1.35 0.09 ⫺0.40 0.06 1.57 0.10 3.45 0.23
9 Concentrate easily 1.38 0.09 ⫺1.76 0.11 0.16 0.05 1.96 0.11
12 Careful thinker 1.65 0.10 ⫺0.81 0.06 0.99 0.06 3.08 0.18
13 Plan for job security 1.01 0.07 ⫺0.92 0.09 0.69 0.08 2.26 0.16
14 Say things 1.10 0.08 ⫺1.15 0.10 1.49 0.11 3.27 0.23
17 Act on impulse 1.49 0.10 ⫺1.04 0.07 1.16 0.07 2.79 0.16
19 Spur of moment 1.40 0.09 ⫺1.54 0.10 0.95 0.07 2.61 0.15
20 Steady thinker 1.59 0.10 ⫺1.40 0.09 0.63 0.06 2.79 0.16
22 Buy on impulse 0.78 0.07 ⫺1.82 0.17 0.97 0.11 3.29 0.28
Note. BIS-11 ⫽ Barratt Impulsiveness Scale-11.
219
BARRATT IMPULSIVENESS SCALE–BRIEF

accounts for the LD in the item analysis without altering the
calculation of the summed score.
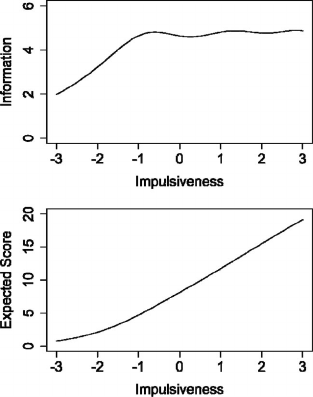
The test information curve is shown in the upper panel of Figure
1. Test information curves show how well the construct is mea-
sured at all levels of the underlying construct continuum. Mea-
surement precision is approximately constant for values of the
construct continuum between –1 and ⫹ 3. Total information for
the eight BIS items is approximately 5 for this range of the
continuum. The standard errors of IRT scores for this range are
approximately
1
兹
5
⫽ 0.45; this translates to an IRT approxima-
tion of reliability of .80 (calculated as one minus measurement
variance) for the eight-item BIS-Brief scores in that range. For
comparison, the traditional reliability estimates using Cronbach’s
alpha for the 30-item BIS-11 and the eight-item BIS-Brief scores
are .83 and .78, respectively. The lower panel of Figure 1 presents
the expected score curve (also known as the test characteristic
curve). This curve shows the expected summed score for each
value of the underlying construct continuum. The curve is linear
for values of impulsiveness on the continuum between ⫺2 and ⫹3;
this implies that the traditional summed score is a good approxi-
mation of the IRT scale score.
Using the methods of IRT, we have developed an eight-item
brief version of the BIS. The next step is to investigate evidence of
construct validity. In Study 2, we evaluated whether scores ob-
tained on the brief version replicate group differences and patterns
of correlations with other psychological constructs that have been
previously found with the 30-item BIS-11 scores.
Study 2: Construct Validation
The construct validity of scores obtained on the BIS-Brief
was investigated using constructs that have been theoretically
and empirically linked with impulsiveness. First, we examined
the capacity of the BIS-Brief to distinguish between female
adults with and without BPD. BPD is a severe mental health
condition characterized by deficits in multiple areas of func-
tioning in the cognitive, affective, and behavioral domains. The
Diagnostic and Statistical Manual of Mental Disorders, fourth
edition, text revision (DSM–IV–TR; American Psychiatric
Association, 2000) requires that five out of nine clinical
symptoms are present for a full diagnosis of BPD, of which one
criteria specifically refers to impulsiveness: impulsivity in at
least two areas that are potentially self-damaging (e.g., spend-
ing, sex, substance abuse, reckless driving, binge eating). A
large number of empirical studies have demonstrated the rela-
tion between borderline traits and impulsivity (Skodol, Gunder-
son, et al., 2002; Skodol, Siever, et al., 2002). We evaluated
whether the BIS-Brief would perform as well as the full BIS-11
in distinguishing patients diagnosed with BPD from normal
controls.
Next, we examined the relation between the BIS-Brief and
aggression-related constructs with data obtained in two separate
samples. Aggressive individuals, and particularly those charac-
terized as impulsively aggressive, have been shown to have
higher scores on personality measures of impulsiveness (Hous-
ton & Stanford, 2005). On this basis, we expected a positive
correlation between the new BIS-Brief and the Impulsive sub-
scale (but not the Premeditated subscale) of the Impulsive
Premeditated Aggression Scale (IPAS; Stanford et al., 2003).
We also expected a positive correlation with anger, hostility,
and aggression as measured by the Buss-Perry Aggression
Questionnaire (BPAQ; Buss & Perry, 1992). All of the data
reported in Study 2 had IRB approval from the respective
universities conducting the data collection.
Table 3
Graded Model Item Parameter Estimates for the Eight BIS-11 Items
Item Content aSE b
1
SE b
2
SE b
3
SE
1 I plan tasks carefully. 1.38 0.09 ⫺1.07 0.08 0.62 0.06 2.96 0.19
2 I do things without thinking. 1.59 0.12 ⫺0.66 0.06 1.58 0.09 3.21 0.21
5 I don’t “pay attention.” 1.17 0.09 ⫺0.82 0.08 1.63 0.11 3.55 0.25
8 I am self-controlled. 1.47 0.10 ⫺0.38 0.06 1.51 0.09 3.29 0.22
9 I concentrate easily. 1.44 0.10 ⫺1.72 0.11 0.16 0.05 1.92 0.11
12 I am a careful thinker. 1.66 0.11 ⫺0.81 0.06 1.00 0.07 3.09 0.19
14 I say things without thinking. 1.15 0.09 ⫺1.12 0.09 1.46 0.11 3.18 0.22
19 I act on the spur of the moment. 1.13 0.09 ⫺1.76 0.13 1.08 0.09 3.01 0.21
Note. BIS-11 ⫽ Barratt Impulsiveness Scale-11.
Table 4
Graded Model Item Parameter Estimates for the BIS-Brief Items, Using a Testlet Combining Items 5 and 9
Item Brief content aSE b
1
SE b
2
SE b
3
SE b
4
SE b
5
SE b
6
SE
1 Plan tasks 1.40 0.10 ⫺1.06 0.08 0.61 0.06 2.93 0.18
2 Do things 1.71 0.12 ⫺0.64 0.06 1.52 0.09 3.08 0.19
8 Self-controlled 1.41 0.10 ⫺0.39 0.06 1.54 0.10 3.36 0.23
12 Careful thinker 1.67 0.12 ⫺0.80 0.06 1.00 0.07 3.08 0.19
14 Say things 1.19 0.09 ⫺1.09 0.09 1.42 0.10 3.10 0.21
19 Spur of moment 1.18 0.09 ⫺1.71 0.12 1.05 0.08 2.92 0.20
5 & 9 Testlet5plus9 1.38 0.09 ⫺2.21 0.13 ⫺0.87 0.07 0.27 0.06 1.47 0.09 2.42 0.14 3.77 0.26
Note. BIS-Brief ⫽ brief version of the Barratt Impulsiveness Scale.
220
STEINBERG, SHARP, STANFORD, AND THARP
Participants
Adult community sample: Borderline versus normal
controls. Participants (N ⫽ 236) were recruited as part of a
larger study evaluating behavioral and neural correlates of social
exchange among healthy controls and individuals diagnosed with
BPD (King-Casas et al., 2008; Patel et al., 2011). Participants were
women from an urban Southwestern city recruited by newspaper
advertisements and pamphlets seeking participants for a study of
individuals with past and current difficulties with intense emo-
tions, relationships, and impulsivity. Of the full sample, n ⫽ 68
(28.8%) met criteria for BPD, whereas n ⫽ 128 (54.2%) were free
of both Axis I (determined by the Structured Clinical Interview for
DSM Disorders; First, Spitzer, Gibbon, & Williams, 2002) and
Axis II disorders (determined by the Diagnostic Interview Sched-
ule for DSM–IV Personality Disorders; DIPD; Zanarini, Franken-
burg, Sickel, & Yong, 1996).
Participants had a mean age of 31.27 years (SD ⫽ 9.8; range ⫽
18 – 63 years). They were primarily Caucasian (46.6%), with a
wide distribution among Black American (19.5%), Hispanic
(19.1%), Asian American (8.9%), and those of mixed race (2.5%);
43.2% of participants reported low annual income (below
$20,000), and 43.6% had never been married.
Adult domestic violence sample. Participants (N ⫽ 111)
were men recently convicted of domestic violence in two south-
eastern Louisiana parishes. Individuals convicted of domestic vi-
olence in these two parishes are court-ordered to attend a state-
approved intervention program as part of sentencing. Recruitment
for the present study occurred during the program’s initial intake
assessment over the course of 12 months. As part of the intake
procedure, participants were asked to participate in the study by
anonymously completing a packet of self-report questionnaires.
The packets were completed at home and returned during the next
appointment. All participants given packets during this time period
returned the packets at least partially completed. Participants had
a mean age of 34.56 years (SD ⫽ 10.87; range ⫽ 18 –71 years).
Adolescent and young adult inpatient sample. The sample
included 92 inpatients in the Adolescent and Young Adult Treat-
ment Programs of a private tertiary care inpatient treatment facility
specializing in the evaluation and stabilization of patients who
failed to respond to previous interventions. All patients on the units
were invited to participate. Exclusion criteria included active psy-
chosis, IQ ⬍ 70, diagnosis of autism spectrum disorder, and for
primary language not being English.
Respondents were between the ages of 13 and 22 (mean age ⫽
16.72; SD ⫽ 2.36). All patients received a comprehensive psychi-
atric evaluation at intake. The modal number of diagnoses was
two, and the average number of diagnoses was between two and
three.
Measures
Adult community sample: Borderline versus normal
controls. The Diagnostic Interview for DSM–IV Personality
Disorders–Borderline Scale (DIPD-BPD; Zanarini et al., 1996)is
a semistructured interview used to diagnose Axis II disorders. The
DIPD-BPD consists of nine items corresponding with DSM–IV
criteria rated as 0 (Not present),1(Possibly present), or 2 (Defi-
nitely present). Five ratings of 2 are necessary to meet criteria for
BPD. The DIPD-BPD has been shown to be a reliable and stable
measure of BPD and has demonstrated strong concurrent validity
(Zanarini et al., 1996, 2003). All interviews were video-recorded
with permission from study participants. To determine each rater’s
agreement with the original diagnostic classification, the video
recordings of 19 participants (17% of the total sample) were
viewed and coded by two trained and independent raters blind to
the group status of participants. Kappa was .88 (p ⬍ .001) for the
first rater, indicating near perfect agreement, and .79 (p ⬍ .001) for
the second rater, indicating substantial agreement (Landis & Koch,
1977). Cronbach’s alpha for the nine items was .89 in the present
sample.
Adult domestic violence sample. Measures included in this
study relevant for the evaluation of the BIS-Brief were the Per-
sonality Assessment Inventory-Borderline subscale (PAI-BOR),
the PAI-Anti-Social subscale (PAI-ANT), the PAI-Aggressive
subscale (PAI-AGG), and the BPAQ (Buss & Perry, 1992).
The PAI (Morey, 1991) includes 344 four-point Likert scale
questions. In addition to assessing the presence of Axis I condi-
tions, it assesses features of paranoid, schizotypal, schizoid, bor-
derline, and antisocial personality disorders. It also includes va-
lidity scales and scales to assist in treatment. The PAI was normed
on a sample of over 3,500 individuals from community, college,
and clinical settings, and internal consistency estimates range from
.75 to .79 for individual scales (Morey, 1991). The PAI-BOR and
the PAI-ANT are two subscales of the PAI that assess symptoms
of personality disorder. The PAI-BOR, in particular, has demon-
strated good internal consistency (Morey, 1991) and construct
validity (Jacobo, Blais, Baity, & Harley, 2007; Kurtz, Morey, &
Tomarken, 1993). Similarly, the PAI-ANT has demonstrated good
internal consistency in the original validation study of the PAI
(Morey, 1991) and strong correlations with the Minnesota Multi-
phasic Personality Inventory scale for antisocial personality disor-
der (Morey, Waugh, & Blashfield, 1985) and the Psychopathy
Figure 1. Upper panel: Test information curve for the Barrat Impulsive-
ness Scale-Brief (BIS-Brief) showing how well the construct is measured
at all levels of the underlying construct continuum. Lower panel: Expected
score curve for the BIS-Brief showing the expected summed score for each
value of the construct continuum.
221
BARRATT IMPULSIVENESS SCALE–BRIEF

Checklist Revised total score (Loranger, Susman, Oldham, &
Russakoff, 1987). The PAI-AGG is a treatment consideration
subscale of the PAI and provides an indicator of potential treat-
ment complications for the clinician using the PAI. The PAI-AGG
has demonstrated good internal consistency and concurrent valid-
ity with the State-Trait Anger Expression Inventory (Morey,
1991).
The BPAQ is a 29-item measure that contains four subscales:
Verbal Aggression (five items; e.g., “My friends say that I’m
somewhat argumentative”; Cronbach’s ␣⫽.80), Physical Aggres-
sion (nine items; e.g., “I get into fights a little more than the
average person”; Cronbach’s ␣⫽.84), Anger (seven items; e.g., “I
have trouble controlling my temper”; Cronbach’s ␣⫽.76), and
Hostility (eight items; e.g., “I am suspicious of overly friendly
strangers”; Cronbach’s ␣⫽.83). Participants responded to items
on a 5-point Likert-type scale, where 1 ⫽ Extremely Uncharac-
teristic of Me and 5 ⫽ Extremely Characteristic of Me. The Anger
and Hostility subscales assess the emotional aspects of aggression.
In past work, anger has been associated with reactive and impul-
sive aggression, and hostility has been associated with premedi-
tated aggression (Stanford et al., 2003).
Adolescent and young adult inpatient sample. Measures
used in this study for evaluation of the BIS-Brief included the
IPAS (Stanford et al., 2003) and the BPAQ (Buss & Perry, 1992).
Here, we describe only the IPAS because the BPAQ was described
above. The IPAS is a 30-item measure that classifies an individ-
ual’s aggressive acts. The IPAS asks participants to consider their
aggressive acts over the past 6 months and then indicate their
agreement (from 5 ⫽ Strongly Agree to 0 ⫽ Strongly Disagree) for
each item on a 5-point Likert-type scale. Traditionally, a screening
question is used (“Over the past 6 months, have you had episodes
where you would become angry and enraged with other people and
acted in an aggressive way?”), and only participants who answer
affirmatively complete the IPAS items. In the present study, we
omitted the screening question so that all participants were asked
to respond to the entire IPAS. The scoring method for the IPAS
was recently revised to reflect new factor analysis findings and to
allow for a categorical and dimensional scoring approach (Stan-
ford, 2011). The new scoring method uses 18 of the 30 IPAS items.
A dimensional approach was used in the present study. Two
subscales are measured: Impulsive Aggression (10 items; e.g.,
“When angry, I reacted without thinking”) and Premeditated Ag-
gression (eight items; e.g., “I felt my outbursts were justified”). In
the dimensional approach, the sum of the item responses in each
subscale is calculated. The IPAS subscale scores had Cronbach’s
alphas of .92 and .85 for Impulsive and Premeditated, respectively.
Results
Adult community sample: Borderline versus normal
controls. Past research has shown that BPD is associated with
higher levels of impulsiveness compared with normal control
samples (Skodol, Gunderson, et al., 2002; Skodol, Siever, et al.,
2002). We performed two independent samples t tests to evaluate
the group differences in impulsiveness between those who met the
criteria for BPD and those who were free of both Axis I and Axis
II disorders. For those who met the criteria for BPD, reliability
estimated with Cronbach’s alpha was .84 and .81 for the 30-item
BIS-11 scores and the eight-item BIS-Brief scores, respectively.
For those free of both Axis I and Axis II disorders, reliability
estimates using Cronbach’s alpha were .81 and .73 for the 30-item
BIS-11 and the eight-item BIS-Brief, respectively. Impulsiveness
scores based on the 30-item BIS-11 showed significant group
mean differences, t(218) ⫽ 16.36, p ⬍ .001; individuals with BPD
had significantly higher scores (M ⫽ 79.63, SD ⫽ 12.02) com-
pared with normal controls (M ⫽ 54.99, SD ⫽ 8.88). These
differences were replicated with the eight-item BIS-Brief, t(227) ⫽
16.29, p ⬍ .001. The BPD group had significantly higher impul-
siveness scores (M ⫽ 21.77, SD ⫽ 4.15) compared with the normal
control group (M ⫽ 13.49, SD ⫽ 3.09). Thus, scores obtained with
the BIS-Brief are found to show the expected group differences in
impulsiveness previously demonstrated with scores based on the
entire 30-item BIS-11.
Adult domestic violence sample. Research has shown that
BIS-11 scores are related to scores obtained on measures of
aggression, hostility, anger, impulsive aggression, antisocial be-
havior, and BPD. We investigated whether the pattern of relation-
ships among these variables is replicated with the eight-item
BIS-Brief using an adult domestic violence sample. For this sam-
ple, reliability estimates using Cronbach’s alpha for the 30-item
BIS-11 scores and the eight-item BIS-Brief scores were .78 and
.74, respectively. Scores obtained on the BIS-11 and BIS-Brief
were divided by their respective numbers of items to place the
scores on the same scale prior to analysis. Table 5 presents the
means and standard deviations of the BIS-11 and the BIS-Brief
and their correlations with the BPAQ Physical Aggression, Verbal
Aggression, Anger, and Hostility subscales and the PAI Border-
line, Antisocial, and Aggression subscales (based on 90 respon-
dents with complete data on the measures). Scores obtained on
these measures that are significantly related to the BIS-11 scores
(i.e., BPAQ Physical, Anger, and Hostility subscales and PAI
Borderline, Antisocial, and Aggression subscales) are also signif-
Table 5
Domestic Violence Sample and Correlations of BIS-11 and BIS-Brief With Buss-Perry and PAI Subscales
Correlation
Measure M (SD) BP-Physical BP-Verbal BP-Anger BP-Hostility PAI-BOR PAI-ANT PAI-AGG
BIS-11 2.12 (0.35) .45 .19 .53 .41 .58 .49 .44
BIS-Brief 2.05 (0.57) .38 .16 .52 .33 .46 .38 .45
Note. BIS-11 ⫽ Barratt Impulsiveness Scale-11; BIS-Brief ⫽ brief version of the Barratt Impulsiveness Scale; BP ⫽ Buss-Perry Aggression
Questionnaire; PAI ⫽ Personality Assessment Inventory; BOR ⫽ Borderline subscale; ANT ⫽ Anti-Social subscale; AGG ⫽ Aggressive subscale. All
correlations are significant at p ⬍ .001, except correlations of BP-Verbal with BIS-11 and BIS-Brief, which are not significant.
222
STEINBERG, SHARP, STANFORD, AND THARP

icantly related to the BIS-Brief scores. Thus, the pattern of corre-
lations observed with the BIS-11 is replicated with the BIS-Brief.
Adolescent and young adult inpatient sample. We investi-
gated whether the pattern of correlations between measures of
aggression (verbal, physical, anger, hostility, impulsive, and pre-
meditated) and the BIS-11 is replicated with the BIS-Brief using
scores obtained from an adolescent and young adult inpatient
sample. For this sample, reliability estimates using Cronbach’s
alpha for the 30-item BIS-11 scores and the eight-item BIS-Brief
scores are .86 and .83, respectively. Before conducting the analy-
ses, the scores obtained on the BIS-11 and the BIS-Brief were
transformed to be on the same scale by dividing each respective
score by its number of items. Table 6 provides the means and
standard deviations of the BIS-11 and the BIS-Brief and their
correlations with the BPAQ subscales and the IPAS subscales
(based on 84 respondents with complete data on the measures). As
shown in the table, scores obtained on these measures that are
significantly related to the BIS-11 (i.e., BPAQ Physical, Verbal,
Anger, and Hostility subscales and the IPAS Impulsive subscale)
are also significantly related to the BIS-Brief. Thus, the relations
observed with the BIS-11 scores and scores from these measures
of aggression are mirrored with scores obtained with the BIS-
Brief.
Discussion
The first aim of the present study was to examine the established
three-factor structure of the BIS through a confirmatory multidi-
mensional IRT approach (Study 1). In anticipation of the shorten-
ing of the BIS, our second aim was to evaluate the construct
validity of scores obtained with the new shorter BIS by examining
its performance against the original 30-item BIS-11 version in
three samples (Study 2). In Study 1, we found that the BIS-11 item
set is multidimensional. However, close inspection of the pattern
of slope parameters show that the BIS-11 exhibits a type of
multidimensionality that is more LD than measurement of indi-
vidual differences on intended psychological constructs. In addi-
tion, fewer than half of the items had substantial slope parameters
on the general factor. These findings led us to develop a short
unidimensional version of the BIS comprised of eight of the
original 30 items.
Barratt originally conceptualized impulsiveness as a unidimen-
sional construct but later, based on the factor analytic studies,
became convinced that impulsiveness encompassed three subtraits
(attentional, motor, and non-planning; Stanford et al., 2009). Al-
though the BIS total sum score rather than subscale scores is most
often used, past research has shown meaningful differences using
these three subscales. For example, Swann et al. (2008) reported
correlations of the three subscales with a sample of patients with
mood disorders and found different relationships between BIS
subscales depending on affective state. Specifically, attentional
impulsiveness was related to both depression and mania, whereas
motor impulsiveness was related to mania, and non-planning im-
pulsiveness was related to depression. A question arises: If mean-
ingful differences like those presented in Swann et al. are found
with the subscale scores, then why were these not interpreted as
“constructs” in the bifactor model? As presented in Table 1, the
slope parameters for the three subscales, listed in columns a
2
–a
4
,
show that for each subscale, two items have substantial slopes,
whereas the remaining items have very small, albeit nonzero
slopes, indicating little relation of the item response to an under-
lying construct. The similarity of content of the items with sub-
stantial slopes on each subscale led to an interpretation of LD,
rather than a meaningful construct on which to measure individual
differences. So, the subscale differences are primarily due to
responses to the two questions with substantial loadings; the re-
maining items contribute some small systematic variability, but
mostly add to measurement error. Thus, the differences that Swann
et al. describe may be mostly a function of individual differences
in responses to the doublets found on each subscale. Although this
requires empirical investigation, it is possible that responses to
these item-doublets are differentially responsive depending on
clinical diagnosis.
In Study 2, we demonstrated similar indices of construct validity
for scores obtained on the BIS-Brief that is found with BIS-11 total
scores using a fraction of the items. Comparing a group diagnosed
with BPD with a normal control group, the BIS-Brief scores
showed the significant group mean difference that was observed
with the BIS-11. In an adult domestic violence sample, the pattern
of correlations of scores obtained with the BIS-11 with measures
of aggression, BPD, and antisocial behavior were replicated with
the BIS-Brief. Using data collected at an inpatient sample of
adolescents and young adults, the pattern of correlations of the
BIS-11 with measures of aggression and impulsive aggression
were found with the BIS-Brief. Our evidence of construct validity
implies that across three different samples and diverse age ranges,
the scores obtained on the BIS-Brief show similar group differ-
ences and patterns of correlations that are observed with the
original 30-item BIS-11 total score. Thus, the eight-item unidi-
mensional BIS-Brief allows for the measurement of impulsiveness
with greater efficiency. This will be useful in clinical assessment
Table 6
Adolescent and Young Adult Inpatient Sample, Correlations of BIS-11 and BIS-Brief With Buss-Perry Aggression Questionnaire, and
Impulsive Premeditated Aggression Scale
Correlation
Measure M (SD) BP-Physical BP-Verbal BP-Anger BP-Hostility IPAS-Impulsive IPAS-Premeditated
BIS-11 2.43 (0.43) .39 .49 .41 .62 .46 .20
BIS-Brief 2.57 (0.65) .34 .48 .36 .53 .37 .17
Note. BIS-11 ⫽ Barratt Impulsiveness Scale-11; BIS-Brief ⫽ brief version of the Barratt Impulsiveness Scale; BP ⫽ Buss-Perry Aggression
Questionnaire; IPAS ⫽ Impulsive Premeditated Aggression Scale. All correlations are significant at p ⫽ .001 or less, except correlations of IPAS-
Premeditated with BIS-11 and BIS-Brief, which are not significant.
223
BARRATT IMPULSIVENESS SCALE–BRIEF
settings as well as large epidemiological studies or intervention
trials of psychiatric disorders.
The findings of the present study have implications for the
conceptualization of impulsiveness. Specifically, a question re-
mains regarding the utility of the cognitive, motor, and non-
planning components of impulsivity. Although our analyses did
not support this conceptualization, variations in the nature of
impulsivity may exist across clinical disorders similar to those
reported in Swann et al. (2008). Although the BIS-11 is not the
most useful instrument to use when examining such variation, it is
possible that instruments specifically designed to measure the
more narrowly defined components of impulsiveness may detect
what differences, if any, exist in impulsiveness across clinical
disorders.
The present study also has implications for the measurement of
psychological constructs. Many instruments presently in use in
clinical, personality, and other areas of psychology were devel-
oped in the 1960s and 1970s and are quite lengthy. At that time,
reliability was a first consideration, and one strategy for increasing
reliability is to increase the number of items. This focus on
reliability leads to the inclusion of many items, some of which are
likely to be repetitious (and this can now be diagnosed with large
LD indices). In addition, when writing items, it becomes increas-
ingly difficult to generate good items; thus, as more items are
written, they are likely to stray from the central theme of the
construct. Present methodology allowed us to (a) distinguish LD
from substantive constructs and (b) reduce the length of the in-
strument by selecting items on the basis of IRT item parameters
and content considerations without loss of information.
One of the implications from this research is that clinical,
personality, and other areas of psychology that rely on the mea-
surement of psychological constructs may benefit if analyses sim-
ilar to that undertaken with the BIS-11 were conducted with many
of the instruments presently in use. Such instruments can poten-
tially be made much shorter. In addition, the evaluation of con-
struct validity of the shorter measure is facilitated because existing
data can be used to compare the mean differences or relationships
between original instruments with other relevant variables and
investigate whether the same group differences or relationships are
observed with new short measures. However, this strategy has its
limitations; for example, this approach precludes any revisions or
additions to the original set of items. As noted previously, some
BIS-11 items were eliminated because the meaning of the item
either drifted from its 1969 meaning (e.g., “I plan for job security”)
or the item lost meaning (e.g., “I am a steady thinker”). Depending
on an evaluation of item quality, for some instruments, it might be
better to develop a measure that includes both legacy items as well
as newly written items. In these cases, new investigations of
evidence of construct validity would be required.
Limitations
The BIS-Brief provides researchers with a short unidimensional
assessment of general impulsiveness that will be particularly use-
ful when the number of questions must be limited, as in large
epidemiological studies, clinical assessment settings, and other
research in which reduction in time and burden on respondents is
desired. The eight-item BIS-Brief score has reliability estimates
comparable to the 30-item BIS-11 total score and shows similar
evidence of construct validity. Notwithstanding these strengths, it
should be noted that use of the BIS-Brief, because it is a unidi-
mensional measure of general impulsiveness, precludes investiga-
tion of the utility of the more narrowly conceptualized specific
components of impulsiveness (e.g., cognitive, planning, behavior).
Much research has been conducted that conceptualizes impulsive-
ness as multidimensional, thus not preserving the specific factors
in the BIS-Brief may limit its usefulness; for example, predictive
relationships that differ among the specific components cannot be
detected by such a general measure. Our goal was to retain a short
form of a general impulsiveness scale, rather than a more specific
or multidimensional scale. Research focused on specific compo-
nents of impulsiveness will require additional measures.
In conclusion, the BIS has had a long and dynamic develop-
mental history (Patton & Stanford, 2011). Originally containing 80
true–false items (Barratt, 1959), the instrument has changed dra-
matically over its 11 revisions. Barratt’s goal was always to
develop the most psychometrically reliable and valid instrument
possible. We see the present study and the BIS-Brief as a contin-
uation of that long developmental process. We suggest that the
BIS-Brief not be seen as a replacement for the BIS-11, but rather
a refinement of the scale much like the BIS-11 was an improve-
ment over its predecessor the BIS-10 (Barratt, 1985). It is our hope
that this next step in the development of the BIS will facilitate even
more work with the instrument for years to come.
References
Ainslie, G. (1975). Specious reward: A behavioral theory of impulsiveness
and impulse control. Psychological Bulletin, 82, 463– 496. doi:10.1037/
h0076860
American Psychiatric Association. (2000). Diagnostic and statistical man-
ual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Barratt, E. S. (1959). Anxiety and impulsiveness related to psychomotor
efficiency. Perceptual and Motor Skills, 9, 191–198. doi:10.2466/pms
.1959.9.3.191
Barratt, E. S. (1985). Impulsiveness subtraits: Arousal and information
processing. In J. T. Spence & C. E. Izard (Eds.), Motivation, emotion,
and personality (pp. 137–146). North Holland, the Netherlands:
Elsevier.
Barratt, E. S., Stanford, M. S., Kent, T. A., & Felthous, A. (1997).
Neuropsychological and cognitive psychophysiological substrates of
impulsive aggression. Biological Psychiatry, 41, 1045–1061. doi:
10.1016/S0006-3223(96)00175-8
Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and
pathological gambling. Addiction, 97, 487– 499. doi:10.1046/j.1360-
0443.2002.00015.x
Brady, K. T., Myrick, H., & McElroy, S. (1998). The relationship between
substance use disorders, impulse control disorders, and pathological
aggression. American Journal of Addiction, 7, 221–230.
Buss, A. H., & Perry, M. P. (1992). The aggression questionnaire. Journal
of Personality and Social Psychology, 63, 452– 459. doi:10.1037/0022-
3514.63.3.452
Cai, L., du Toit, S. H. C., & Thissen, D. (2011). IRTPRO: Flexible,
multidimensional, multiple categorical IRT modeling [Computer soft-
ware]. Chicago, IL: Scientific Software International.
Cai, L., Maydeu-Olivares, A., Coffman, D. L., & Thissen, D. (2006).
Limited information goodness-of-fit testing of item response theory
models for sparse 2
p
tables. British Journal of Mathematical and Sta
-
tistical Psychology, 59, 173–194. doi:10.1348/000711005X66419
224
STEINBERG, SHARP, STANFORD, AND THARP
Cai, L., Yang, J. S., & Hansen, M. (2011). Generalized full-information
item bifactor analysis. Psychological Methods, 16, 221–248. doi:
10.1037/a0023350
Chen, W.-H., & Thissen, D. (1997). Local dependence indices for item
pairs using item response theory. Journal of Educational and Behavioral
Statistics, 22, 265–289.
de Wit, H. (2009). Impulsivity as a determinant and consequence of drug
use: A review of underlying processes. Addiction Biology, 14, 22–31.
doi:10.1111/j.1369-1600.2008.00129.x
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (2002).
Structured Clinical Interview for DSM–IV–TR Axis I Disorders: Re-
search version, patient edition (SCID-I/P). New York, NY: Biometrics
Research, New York State Psychiatric Institute.
Fraley, R. C., Waller, N. G., & Brennan, K. A. (2000). An item response
theory analysis of self-report measures of adult attachment. Journal of
Personality and Social Psychology, 78, 350 –365. doi:10.1037/0022-
3514.78.2.350
Gibbons, R. D., Weiss, D. J., Kupfer, D. J., Frank, E., Fagoilini, A.,
Grochocinski, V. J.,...Immekus, J. C. (2008). Using computerized
adaptive testing to reduce the burden of mental health assessment.
Psychiatric Services, 59, 361–368. doi:10.1176/appi.ps.59.4.361
Gray, J. A. (1987). Perspectives on anxiety and impulsivity: A commen-
tary. Journal of Research in Personality, 21, 493–509. doi:10.1016/
0092-6566(87)90036-5
Gray-Little, B., Williams, V. S. L., & Hancock, T. D. (1997). An item
response theory analysis of the Rosenberg Self-Esteem Scale. Person-
ality and Social Psychology Bulletin, 23, 443– 451. doi:10.1177/
0146167297235001
Houston, R. J., & Stanford, M. S. (2005). Electrophysiological substrates
of impulsiveness: Potential effects on aggressive behavior. Progress in
Neuro-Psychopharmacology and Biological Psychiatry, 29, 305–313.
doi:10.1016/j.pnpbp.2004.11.016
Ireland, J. L., & Archer, J. (2008). A confirmatory factor analysis study of
the Barratt Impulsivity Scale. Personality and Individual Differences,
45, 286 –292. doi:10.1016/j.paid.2008.04.012
Jacobo, M. C., Blais, M. A., Baity, M. R., & Harley, R. (2007). Concurrent
validity of the Personality Assessment Inventory borderline scales in
patients seeking dialectical behavior therapy. Journal of Personality
Assessment, 88, 74 –80.
King-Casas, B., Sharp, C., Lomax, L., Lohrenz, T., Fonagy, P., & Mon-
tague, R. (2008, August 8). The rupture and repair of cooperation in
borderline personality disorder. Science, 321, 806 – 810. doi:10.1126/
science.1156902
Kurtz, J. E., Morey, L. C., & Tomarken, A. J. (1993). The concurrent
validity of three self-report measures of borderline personality. Journal
of Psychopathology and Behavioral Assessment, 15, 255–266.
Landis, J. R., & Koch, G. G. (1977). The measurement of observer
agreement for categorical data. Biometrics, 33, 159 –174. doi:10.2307/
2529310
Lejuez, C. W., Magisdson, S. H., Mitchell, R. S., Stevens, M. C., & de Wit,
H. (2010). Behavioral and biological indicators of impulsivity in the
development of alcohol use, problems, and disorders. Alcoholism: Clin-
ical and Experimental Research, 34, 1334–1345.
Links, P. S., Heslegrave, R., & van Reekum, R. (1999). Impulsivity: Core
aspect of borderline personality. Journal of Personality Disorders, 13,
1–9. doi:10.1521/pedi.1999.13.1.1
Logan, G. D. (1994). On the ability to inhibit thought and action: A user’s
guide to the stop signal paradigm. Dagenback, and T. H. Carr (Eds.),
Inhibitory processes in attention, memory, and language (pp. 189–239).
San Diego,CA: Academic Press.
Loranger, A. W., Susman, V. L., Oldham, J. M., & Russakoff, L. M.
(1987). The Personality Disorder Examination: A preliminary report.
Journal of Personality Disorders, 1, 1–13. doi:10.1521/pedi.1987.1.1.1
Maydeu-Olivares, A., & Joe, H. (2005). Limited and full information
estimation and goodness-of-fit testing in 2n contingency tables: A uni-
fied framework. Journal of the American Statistical Association, 100,
1009 –1020. doi:10.1198/016214504000002069
Maydeu-Olivares, A., & Joe, H. (2006). Limited information goodness-of-
fit testing in multidimensional contingency tables. Psychometrika, 71,
713–732. doi:10.1007/s11336-005-1295-9
Meda, S. A., Stevens, M. C., Potenza, M. D., Pittman, B., Gueorguieva, R.,
Andrews, M. M.,...Pearlson, G. D. (2009). Investigating the behavioral
and self-report constructs of impulsivity domains using principal com-
ponent analysis. Behavioral Pharmacology, 20, 390 –399. doi:10.1097/
FBP.0b013e32833113a3
Moeller, F. G., Barratt, E. S., Dougherty, D. M., Schmitz, J. M., & Swann,
A. C. (2001). Psychiatric aspects of impulsivity. American Journal of
Psychiatry, 158, 1783–1793. doi:10.1176/appi.ajp.158.11.1783
Morey, L. C. (1991). Personality assessment inventory. Lutz, FL: Psycho-
logical Assessment Resources.
Morey, L. C., Waugh, M. H., & Blashfield, R. K. (1985). MMPI scales for
DSM–III personality disorders: Their derivation and correlates. Journal
of Personality Assessment, 49, 245–251. doi:10.1207/
s15327752jpa4903_5
Nigg, J. T. (2003). Response inhibition and disruptive behaviors: Toward
a multiprocess conception of etiological heterogeneity for ADHD com-
bined type and conduct disorder early-onset type. Annals of the New
York Academy of Sciences, 1008, 170 –182. doi:10.1196/annals.1301
.018
Patel, A., Sharp, C., & Fonagy, P. (2011). Criterion validity of the MSI-
BPD in a community sample of women. Journal of Psychopathology
and Behavioral Assessment, 33, 403–408. doi:10.1007/s10862-011-
9238-5
Patton, J. H., & Stanford, M. S. (2011). Psychology of impulsivity. In J.
Grant & M. Potenza (Eds.), The Oxford handbook of impulse control
disorders (pp. 262–278). New York, NY: Oxford University Press.
Patton, J. H., Stanford, M. S., & Barratt, E. S. (1995). Factor structure
of the Barratt Impulsiveness Scale. Journal of Clinical Psychology,
51, 768–774. doi:10.1002/1097-4679(199511)51:6⬍768::AID-
JCLP2270510607⬎3.0.CO;2-1
Reynolds, B., Ortengren, A., Richards, J. B., & de Wit, H. (2006). Dimen-
sions of impulsive behavior: Personality and behavioral measures. Per-
sonality and Individual Differences, 40, 305–315. doi:10.1016/j.paid
.2005.03.024
Samejima, F. (1969). Estimation of latent ability using a response pattern
of graded scores. Psychometric Monograph Supplement, 34(4, Pt. 2).
Samejima, F. (1997). Graded response model. In W. J. van der Linden &
R. K. Hambleton (Eds.), Handbook of item response theory (pp. 85–
100). New York, NY: Springer-Verlag.
Sharp, C., Ha, C., & Fonagy, P. (2011). Get them before they get you:
Trust, trustworthiness and social cognition in boys with and without
externalizing behavior problems. Development and Psychopathology,
23, 647– 658. doi:10.1017/S0954579410000003
Skodol, A. E., Gunderson, J. G., Pfohl, B., Widiger, T. A., Livesley, W. J.,
& Siever, L. J. (2002). The borderline diagnosis I: Psychopathology,
comorbidity, and personality structure. Biological Psychiatry, 51, 936–
950. doi:10.1016/S0006-3223(02)01324-0
Skodol, A. E., Siever, L. J., Livesley, W. J., Gunderson, J. G., Pfohl, B., &
Widiger, T. A. (2002). The borderline diagnosis II: Biology, genetics,
and clinical course. Biological Psychiatry, 51, 951–963. doi:10.1016/
S0006-3223(02)01325-2
Spinella, M. (2007). Normative data and a short form of the Barratt
Impulsiveness Scale. International Journal of Neuroscience, 117, 359 –
368. doi:10.1080/00207450600588881
Stanford, M. S. (2011). Procedures for the classification of aggressive/
violent acts. Unpublished manuscript.
225
BARRATT IMPULSIVENESS SCALE–BRIEF
Stanford, M. S., Houston, R. J., & Baldridge, R. M. (2008). Comparison of
impulsive and premeditated perpetrators of intimate partner violence.
Behavioral Sciences and the Law, 26, 709 –722. doi:10.1002/bsl.808
Stanford, M. S., Houston, R. J., Mathias, C. W., Villemarette-Pittman,
N. R., Helfritz, L. E., & Conklin, S. M. (2003). Characterizing aggres-
sive behavior. Assessment, 10, 183–190.
Stanford, M. S., Mathias, C. W., Dougherty, D. M., Lake, S. L., Anderson,
N. E., & Patton, J. H. (2009). Fifty years of the Barratt Impulsiveness
Scale: An update and review. Personality and Individual Differences,
47, 385–395. doi:10.1016/j.paid.2009.04.008
Steinberg, L. (1994). Context and serial-order effects in personality mea-
surement: Limits on the generality of measuring changes the measure.
Journal of Personality and Social Psychology, 66, 341–349. doi:
10.1037/0022-3514.66.2.341
Steinberg, L. (2001). The consequences of pairing questions: Context
effects in personality measurement. Journal of Personality and Social
Psychology, 81, 332–342. doi:10.1037/0022-3514.81.2.332
Steinberg, L., & Thissen, D. (1996). Uses of item response theory and the
testlet concept in the measurement of psychopathology. Psychological
Methods, 1, 81–97. doi:10.1037/1082-989X.1.1.81
Swann, A. C., Steinberg, J. L., Lijffijt, M., & Moeller, F. G. (2008).
Impulsivity: Differential relationship to depression and mania in bipolar
disorder. Journal of Affective Disorders, 106, 241–248. doi:10.1016/j
.jad.2007.07.011
Thissen, D. (2009). The MEDPRO project: An SBIR project for a com-
prehensive IRT and CAT software system—IRT software. In D. J. Weiss
(Ed.), Proceedings of the 2009 GMAC Conference on Computerized
Adaptive Testing. Retrieved from www.psych.umn.edu/psylabs/
CATCentral/
Thissen, D., & Steinberg, L. (2010). Using item response theory to disen-
tangle constructs at different levels of generality. In S. Embretson (Ed.),
Measuring psychological constructs: Advances in model-based ap-
proaches (pp. 123–144). Washington, DC: American Psychological
Association. doi:10.1037/12074-006
Whiteside, S. P., & Lynam, D. R. (2001). The Five Factor Model and
impulsivity: Using a structural model of personality to understand im-
pulsivity. Personality and Individual Differences, 30, 669– 689. doi:
10.1016/S0191-8869(00)00064-7
Yung, Y. F., McLeod, L. D., & Thissen, D. (1999). On the relationship
between the higher-order factor model and the hierarchical factor model.
Psychometrika, 64, 113–128. doi:10.1007/BF02294531
Zanarini, M. C., Frankenburg, F. R., Sickel, A. E., & Yong, L. (1996). The
Diagnostic Interview for DSM–IV Personality Disorders (DIPD-IV).
Belmont, MA: McLean Hospital, Laboratory for the Study of Adult
Development.
Zanarini, M. C., Vujanovic, A., Parachini, E. A., Boulanger, J. L., Fran-
kenburg, F. R., & Hennen, J. (2003). A screening measure for BPD: The
McLean Screening Instrument for Borderline Personality Disorder
(MSI-BPD). Journal of Personality Disorders, 17, 568 –573. doi:
10.1521/pedi.17.6.568.25355
Received September 19, 2011
Revision received August 1, 2012
Accepted August 6, 2012 䡲
226
STEINBERG, SHARP, STANFORD, AND THARP
